Cervical nerve roots and the dural sheath: a histological study using human fetuses near term
- Affiliations
-
- 1Department of Histology and Embryology, Tokyo Dental College, Tokyo, Japan
- 2Department of Anatomy, Tokyo Dental College, Tokyo, Japan
- 3Division of Internal Medicine, Jikou-kai Home Visit Clinic, Sapporo, Japan
- KMID: 2509691
- DOI: http://doi.org/10.5115/acb.20.081
Abstract
- We have previously reported that the thoracolumbar posterior nerve root shows a tortuous epidural course, based on studies of human fetuses near term. For comparison with the cervical nerve, examinations were conducted using frontal, sagittal and horizontal sections of cervical vertebrae from 22 fetuses at 30–38 weeks of gestation. The cervical nerve root showed a short, straight and lateral course near the zygapophysial joint. Multiple rather than single bundles of the cervical posterior root seemed to account for the majority of sensory nerve fibers innervating the upper extremity. Fasciculation of rootlets was evident near the thoracolumbar spinal cord, whereas it was seen in the dural pocket at the nerve exit from the dural sac although both sites were subdural. As in the thoracolumbar region, the nerve sheath was continuous with the dura mater and independently surrounded each of the anterior and posterior roots. Radicular arteries were few in the cervical region. In 2 of the 22 fetuses (31 weeks and 33 weeks), there was a segmental, unilateral abnormality of nerve rootlet fasciculation where the dorsal root ganglion was located lateral or peripheral to the intervertebral region. Long nerve roots running inferiorly are a necessary adaptation to the delayed and marked growth of the thoracolumbar vertebral column. In children, the cervical nerve roots are likely to be affected by movement or dislocation of the vertebrae. The segmental abnormality of the cervical nerve root may be linked to rare variations in the brachial plexus.
Keyword
Figure
-
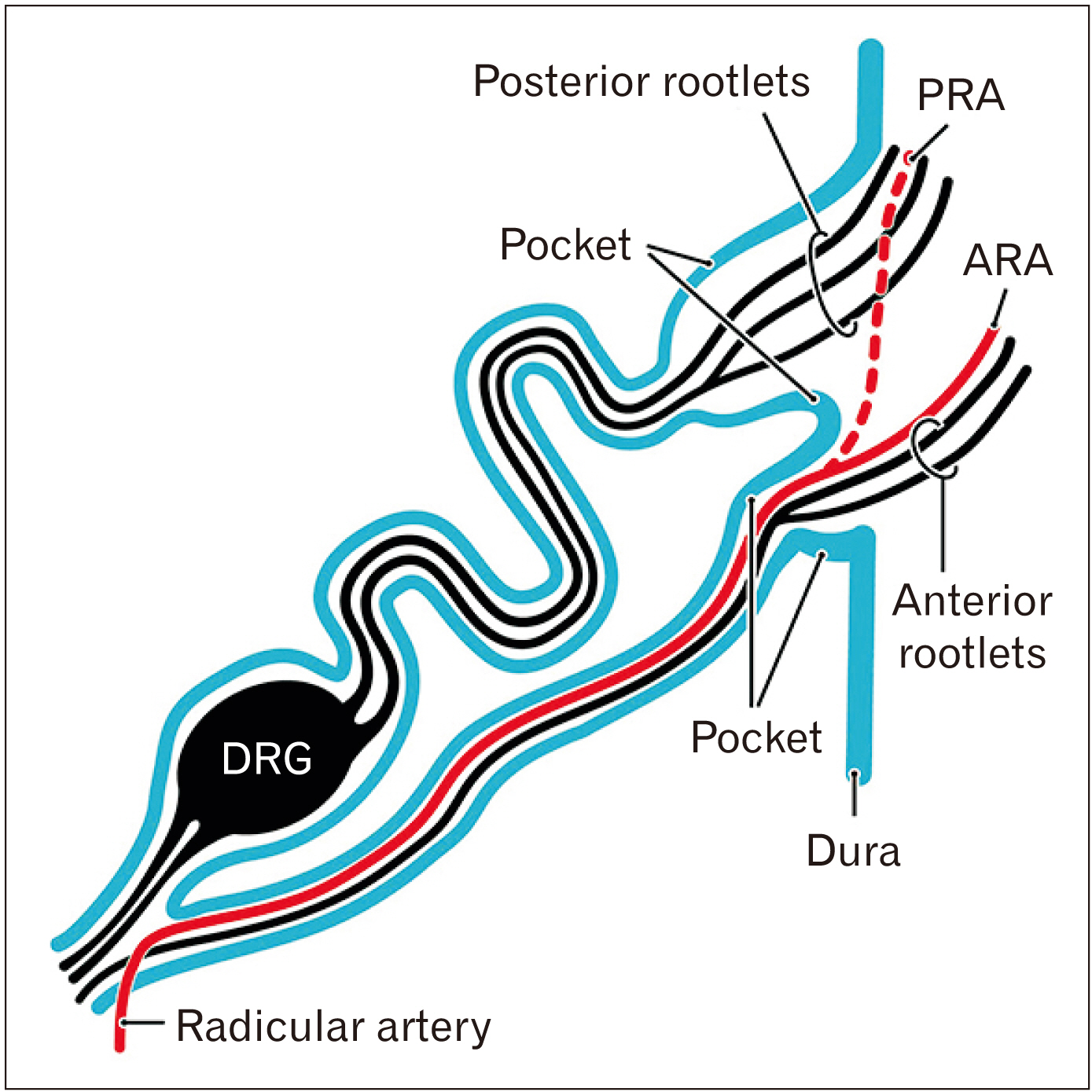
Fig. 1 Diagram of thoracic spinal nerve roots in the human fetus near term. Blue color indicates the dura mater and the nerve sheath continuous with the dura. The posterior and anterior rootlets enter superior and inferior ‘pockets’ of the dura mater, respectively. The posterior root is characterized by a wavy course in contrast to the straight anterior root. A radicular artery, if present at the nerve level, runs along the anterior root and, in the dural pocket, decides the direction along the posterior or anterior rootlets, i.e., the PRA or ARA. ARA, anterior radicular artery; DRG, dorsal root ganglion; PRA, posterior radicular artery. Modified from Cho et al. Biomed Res Int 2016 Mar 16 [Epub]. http://dx.doi.org/10.1155/2016/8163519 [3].

Fig. 2 Frontal sections of the cervical cord and nerve roots from a fetus measuring 270 mm (OC27). (A) displays the most anterior site in the figure, and (I) the most posterior. Green dots and short lines indicate candidate radicular arteries. Stars indicate the bottom of the dural sac. Higher cervical nerve roots cross the dural sac in more anterior sections: the second and third cervical nerves appear in (A, B), whereas the fifth and/or sixth nerves appear in (F–I). Squares in (A–G) (nerve roots) are shown in Fig. 3 at higher magnification. (A–I) were prepared at the same magnification (scale bar in A, 5 mm). None of the figures show a radicular artery candidate with a longitudinal course (colored green). C1–C6, first-sixth cervical vertebrae; DRG, dorsal root ganglion; OC, occipital basilar part; VA, vertebral artery.

Fig. 3 Cervical nerve roots at the dural sac exit. Higher-magnification views of the squares shown in Fig. 2. Four combinations of figures display the same nerve root: (A, B) second cervical nerve, (C, D) third, (F, G) fourth, and (H, I) fifth. In the second and fifth cervical nerves, the anterior root (N2a in A; N5a in H) crosses the dural sac anterior to the corresponding posterior root (N2p in B; N5p in I). However, in the third and fourth cervical nerves, the anterior and posterior roots cross the sac together (N3a and N3p in D; N4a and N4p in G). The posterior root is usually composed of 2–3 bundles, in contrast to the single bundle of the anterior root. The dural sac forms a pocket-like structure receiving the nerve root (E, G, I). None of the figures show a radicular artery candidate with a longitudinal course (colored green). (A–I) were prepared at the same magnification (scale bar in A, 1 mm). DRG, dorsal root ganglion.

Fig. 4 Sagittal sections of cervical nerve roots from two fetuses near term. (A–D) display sections from a fetus with a CRL of 302 mm (OC26), and (E–H) those from a fetus with a CRL of 285 mm (OC28). (A, E) show the most medial site in the specimen, and (D, H) the most lateral. Stars indicate the bottom of the dural sac. The rootlets are bundled into two nerve roots in (B), and into two or three bundles in (F, G) (higher magnification, see Fig. 5). (A–H) were prepared at the same magnification (scale bar in A, 5 mm). C1, C2, and C6, the first, second and sixth cervical vertebrae; CRL, crown-rump length; DRG, dorsal root ganglion; OC, occipital basilar part; VA, vertebral artery.

Fig. 5 Sagittal sections showing exit of cervical nerve roots from the dural sac to the DRG. Higher-magnification views of the squares shown in Fig. 4. (A–D) show sections from a fetus with a CRL of 302 mm (OC26), and (E–H) those from a fetus with a CRL of 285 mm (OC28). (A, E) show the most medial site in the specimen, and (D, H) the most lateral. The anterior nerve roots of the fourth-seventh cervical nerves (N4a–N7a) are adjacent to the anterior side of the corresponding posterior roots (N4p–N7p) in (B, F). The DRG is surrounded by veins (G). The anterior root can be clearly identified near and around the ganglion (N6a in D, G). The posterior root of the fifth and sixth cervical nerves (N5P, N6p) is composed of 2–3 bundles in (F), in contrast to a single bundle in (C). The pocket of the dural sac at the nerve exit (A, E) is much larger than that seen in frontal sections (Fig. 3G, I). A few radicular artery candidates (colored green) show a longitudinal course (C, G). (A–H) were prepared at the same magnification (scale bar in A, 1 mm). C3–C6, the third-sixth cervical vertebrae; CRL, crown-rump length; VA, vertebral artery.

Fig. 6 Horizontal sections including the sixth cervical nerve root. (A, B, D–F) were prepared at the same magnification (scale bars: 5 mm in A, 1 mm in D). (D–F) are higher-magnification views of the centers of (A–C), respectively. (A, D) display a plane 0.2 mm superior to (C, F). The anterior nerve root (N6a) as well as two bundles of the posterior root (N6p) take an almost straight course and run in parallel. The radicular artery (RA; colored green) takes a longitudinal course accompanying the anterior root in (D, E). C5, C6, the fifth and sixth cervical vertebrae; DRG, dorsal root ganglion; VA, vertebral artery.

Fig. 7 Abnormality restricted to the sixth cervical nerve: sagittal sections from a fetus with a CRL of 280 mm (OC29). (A) shows the most medial site in the specimen, and (I , J) the most lateral. (I) is a higher-magnification view of the central part of (J). (A–H, J) were prepared at the same magnification (scale bars: 5 mm in A; 1 mm in I). Stars indicate the bottom of the dural sac. The fifth and seventh cervical rootlets are bundled into two nerve roots (N5a and N5p, N7a and N7p) in (B–D), but no fasciculation is evident in the sixth nerve (circle in D; higher magnification, see Fig. 7). The DRG of the sixth cervical nerve (N6a, N6p) is absent between the vertebral arches (E, F) but appears laterally between the scalenus muscles (I, J). C1, C2, and C7, the first, second and seventh cervical vertebrae; CRL, crown-rump length; OC, occipital basilar part; VA, vertebral artery.

Fig. 8 Abnormality in the sixth cervical nerve: higher magnification. The same specimen as that shown in Fig. 6. (A) shows a plane slightly lateral to Fig. 6B. (B–D) correspond to the squares in Figs. 6C–E, respectively. (A) contains rootlets of the fourth and fifth cervical nerves (N4, N5) in the dural sac. In (B–D), the anterior nerve roots (N4a, N5a, N6a, N7a) can be discriminated from the dorsal root (N4p, N5p, N6p, N7p). The sixth DRG is absent in (D), which includes ganglia at other levels. None of the figures contain radicular artery candidates showing a longitudinal course (colored green). (A–D) were prepared at the same magnification (scale bar in A, 1 mm). C2, C3, C5, and C6, the second, third, fifth and sixth cervical vertebrae;
Reference
-
References
1. Tubbs RS, Lobashevsky A, Oakes P, D'Antoni AV, Hattab E, Topp K, Loukas M, Spinner R. 2015; Meningeal relationships to the spinal nerves and rootlets: a gross, histological, and radiological study with application to intradural extramedullary spinal tumors. Childs Nerv Syst. 31:675–81. DOI: 10.1007/s00381-015-2648-z. PMID: 25686899.
Article2. Jang HS, Cho KH, Chang H, Jin ZW, Rodriguez-Vazquez JF, Murakami G. 2016; The filum terminale revisited: a histological study in human fetuses. Pediatr Neurosurg. 51:9–19. DOI: 10.1159/000439284. PMID: 26595116.
Article3. Cho KH, Jin ZW, Abe H, Shibata S, Murakami G, Rodríguez-Vázquez JF. 2016; Neural-dural transition at the thoracic and lumbar spinal nerve roots: a histological study of human late-stage fetuses. Biomed Res Int. 2016:8163519. DOI: 10.1155/2016/8163519. PMID: 27069926. PMCID: PMC4812201.
Article4. Yi M, Lee JW, Yeom JS, Joe E, Hong SH, Lee GY, Kang HS. 2014; C2 nerve root on magnetic resonance imaging of occipital neuralgia. Spine (Phila Pa 1976). 39:1077–83. DOI: 10.1097/BRS.0000000000000345. PMID: 24732835.
Article5. O'Rahilly R, Muller F, Meyer DB. 1980; The human vertebral column at the end of the embryonic period proper. 1. The column as a whole. J Anat. 131(Pt 3):565–75. PMID: 7216919. PMCID: PMC1233253.6. Castellana C, Kósa F. 1999; Morphology of the cervical vertebrae in the fetal-neonatal human skeleton. J Anat. 194(Pt 1):147–52. DOI: 10.1046/j.1469-7580.1999.19410147.x. PMID: 10227677. PMCID: PMC1467903.
Article7. Cattell HS, Filtzer DL. 1965; Pseudosubluxation and other normal variations in the cervical spine in children. A study of one hundred and sixty children. J Bone Joint Surg Am. 47:1295–309. DOI: 10.2106/00004623-196547070-00001. PMID: 5837630.8. Bogduk N. 2016; Functional anatomy of the spine. Handb Clin Neurol. 136:675–88. DOI: 10.1016/B978-0-444-53486-6.00032-6. PMID: 27430435.
Article9. San Román P, Palma JC, Oteo MD, Nevado E. 2002; Skeletal maturation determined by cervical vertebrae development. Eur J Orthod. 24:303–11. DOI: 10.1093/ejo/24.3.303. PMID: 12143094.10. Khorooshi MH, Fischer Hansen B, Keeling J, Nolting D, Kjaer I. 2001; Prenatal localization of the dorsal root ganglion in different segments of the normal human vertebral column. Spine (Phila Pa 1976). 26:1–5. DOI: 10.1097/00007632-200101010-00002. PMID: 11148637.
Article11. Müller F, O'Rahilly R. 1986; Somitic-vertebral correlation and vertebral levels in the human embryo. Am J Anat. 177:3–19. DOI: 10.1002/aja.1001770103. PMID: 3535481.
Article12. Müller F, O'Rahilly R. 2003; Segmentation in staged human embryos: the occipitocervical region revisited. J Anat. 203:297–315. DOI: 10.1046/j.1469-7580.2003.00219.x. PMID: 14529047. PMCID: PMC1571167.13. Hashimoto J, Murakami G, Tsugane MH, Chisaka O, Capecchi MR, Ogino T. 1999; Lumbosacral plexus in Hoxa9 knockout mice with special reference to their nerve variations identified according to whether they were interphenotypic or intergenotypic differences. Kaibogaku Zasshi. 74:609–30. PMID: 10659578.14. Bots J, Wijnaendts LC, Delen S, Van Dongen S, Heikinheimo K, Galis F. 2011; Analysis of cervical ribs in a series of human fetuses. J Anat. 219:403–9. DOI: 10.1111/j.1469-7580.2011.01400.x. PMID: 21689099. PMCID: PMC3171776.
Article15. Klika E, Zajícová A. 1976; The development of meninges in chicken embryos. Anat Anz. 140:379–86. PMID: 1023773.16. O'Rahilly R, Müller F. 1986; The meninges in human development. J Neuropathol Exp Neurol. 45:588–608. DOI: 10.1097/00005072-198609000-00008. PMID: 3746345.17. Hunter AG, Seaver LH, Stevenson RE. 2011; Limb-body wall defect. Is there a defensible hypothesis and can it explain all the associated anomalies? Am J Med Genet A. 155A:2045–59. DOI: 10.1002/ajmg.a.34161. PMID: 21815262.
Article18. Raphaeli T, Parimi C, Mattix K, Javid PJ. 2010; Acute colonic obstruction from Ladd bands: a unique complication from intestinal malrotation. J Pediatr Surg. 45:630–1. DOI: 10.1016/j.jpedsurg.2009.12.026. PMID: 20223332.
Article19. Komuro H, Hoshino N, Urita Y, Fujishiro J, Sakamoto N, Ono K, Kaneko M. 2010; Pathogenic implications of remnant vitelline structures in gastroschisis. J Pediatr Surg. 45:2025–9. DOI: 10.1016/j.jpedsurg.2010.04.017. PMID: 20920723.
Article20. Fukuzawa R, Toma M, Nomura A. 2011; Histology of a paraumbilical band in a neonate with gastroschisis. Pediatr Dev Pathol. 14:493–5. DOI: 10.2350/11-06-1053-CR.1. PMID: 21875339.
Article21. Kim JH, Hwang SE, Rodríguez-Vázquez JF, Murakami G, Cho BH. 2014; Liver agenesis with omphalocele: a report of two human embryos using serial histological sections. Pediatr Dev Pathol. 17:431–40. DOI: 10.2350/14-05-1484-OA.1. PMID: 25133969.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Avulsion Injury of Lumbosacral Nerve Roots Associated with Femur Fractures: A case Report
- Primary Malignant Melanoma of the Cervical Spinal Nerve Root
- An Anatomical Study on the Variations of the First Cervical Dorsal Root
- Two Cases of Neurilemmoma of the Cervical Vagus Nerve Including IntracapsularEnucleation of Nerve Preservation
- Neurilemmoma in Cervical Dorsal Nerve Root: A case report
