J Korean Med Sci.
2020 Apr;35(13):e95. 10.3346/jkms.2020.35.e95.
The Utility of the Random Urine Uric Acid-to-Creatinine Ratio for Patients with Gout Who Need Uricosuric Agents: Retrospective Cross-Sectional Study
- Affiliations
-
- 1Division of Rheumatology, Department of Internal Medicine, Chung-Ang University College of Medicine, Seoul, Korea
- 2Division of Nephrology, Department of Internal Medicine, International St. Mary's Hospital, Catholic Kwandong University, Incheon, Korea.
- KMID: 2509602
- DOI: http://doi.org/10.3346/jkms.2020.35.e95
Abstract
- Background
The 24-hour uric acid excretion measurement is important in assessing disease status and helping to select the appropriate uric acid-lowering agent for patients with gout, however, it is inconvenient. The authors investigated the efficacy of the random urine uric acid-to-creatinine (UA/CR) ratio to screen the patients who under-secreted 24-hour urine uric acid.
Methods
This was a retrospective cross-sectional study. Ninety patients with gout, without undergoing uric acid-lowering treatment were enrolled. Twenty-four-hour urine and random urine samples were obtained on the same day. Six hundred mg of uric acid in the 24-hour urine sample was used as a standard for distinguishing between over and under-excretion groups.
Results
The random urinary UA/CR ratio showed positive correlation with 24-hour urine uric acid excretion (γ = 0.398, P < 0.001). All the patients with the random UA/CR less than 0.2 excreted less than 600 mg uric acid in 24-hour urine collection. When the random urine UA/CR ratio < 0.2 was regarded as a positive result, the positive predictive value, negative predictive value, sensitivity, and specificity in the uric acid under-excretion were 100% (8 of 8), 64.6% (53 of 82), 21.6% (8 of 37), and 100% (53 of 53), respectively.
Conclusion
There is a moderate positive correlation between the random urinary UA/CR ratio and 24-hour urine uric acid excretion, so that UA/CR ratio may not be a good predictor of 24-hour urine uric acid excretion. However, the random urine UA/CR ratio 0.2 can be a useful predictor to screen the gouty patients who need to be treated with uricosuric drugs.
Keyword
Figure
-
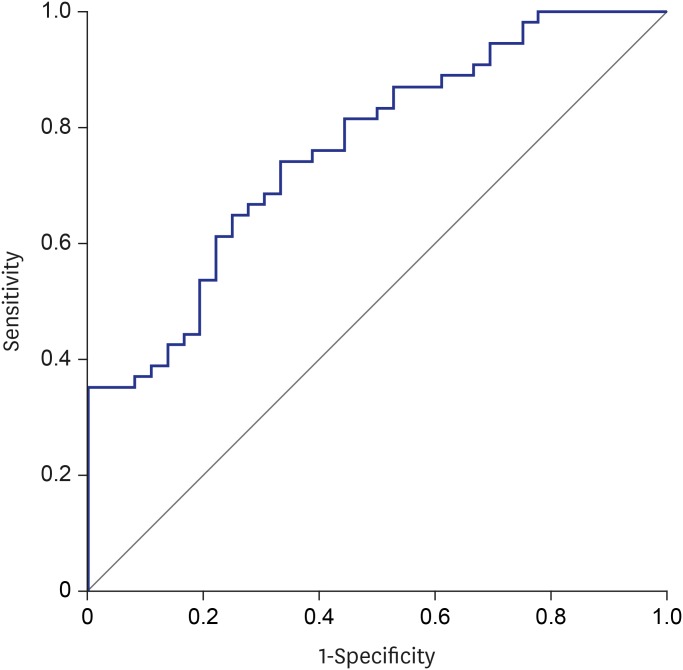
Fig. 1 Receiver operation characteristic curves for the random urine uric acid-to-creatinine ratio to discriminate 24-hour urine uric acid excretion > 600 mg.
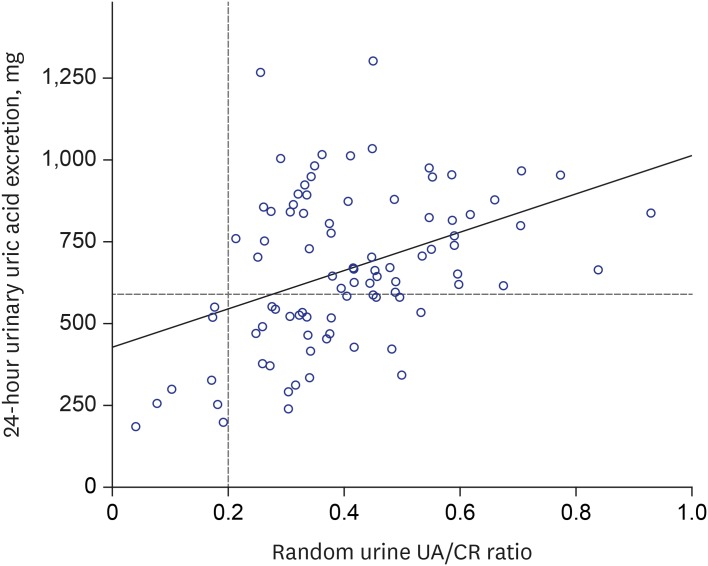
Fig. 2 The correlations between 24-hour urine uric acid excretion and the random urine UA/CR.UA/CR = uric acid-to-creatinine ratio.
Reference
-
1. Khanna D, Fitzgerald JD, Khanna PP, Bae S, Singh MK, Neogi T, et al. 2012 American College of Rheumatology guidelines for management of gout. Part 1: systematic nonpharmacologic and pharmacologic therapeutic approaches to hyperuricemia. Arthritis Care Res (Hoboken). 2012; 64(10):1431–1446. PMID: 23024028.
Article2. Richette P, Doherty M, Pascual E, Barskova V, Becce F, Castañeda-Sanabria J, et al. 2016 updated EULAR evidence-based recommendations for the management of gout. Ann Rheum Dis. 2017; 76(1):29–42. PMID: 27457514.
Article3. Schumacher HR, Chen LX. Gout and other crystal-associated arthropathies. In : Kasper DL, Fauci AS, Hauser SL, Longo DL, Jameson JL, Loscalzo J, editors. Harrison's Principles of Internal Medicine. 19th ed. New York, NY: McGraw-Hill Education;2015. p. 2234.4. Perez-Ruiz F, Hernandez-Baldizon S, Herrero-Beites AM, Gonzalez-Gay MA. Risk factors associated with renal lithiasis during uricosuric treatment of hyperuricemia in patients with gout. Arthritis Care Res (Hoboken). 2010; 62(9):1299–1305. PMID: 20506124.
Article5. Neogi T, Jansen TL, Dalbeth N, Fransen J, Schumacher HR, Berendsen D, et al. 2015 Gout Classification Criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheumatol. 2015; 67(10):2557–2568. PMID: 26352873.
Article6. Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D, et al. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Ann Intern Med. 1999; 130(6):461–470. PMID: 10075613.
Article7. Moriwaki Y, Yamamoto T, Takahashi S, Yamakita J, Tsutsumi Z, Hada T. Spot urine uric acid to creatinine ratio used in the estimation of uric acid excretion in primary gout. J Rheumatol. 2001; 28(6):1306–1310. PMID: 11409124.8. Perez-Ruiz F, Calabozo M, Erauskin GG, Ruibal A, Herrero-Beites AM. Renal underexcretion of uric acid is present in patients with apparent high urinary uric acid output. Arthritis Rheum. 2002; 47(6):610–613. PMID: 12522834.
Article9. Simkin PA, Hoover PL, Paxson CS, Wilson WF. Uric acid excretion: quantitative assessment from spot, midmorning serum and urine samples. Ann Intern Med. 1979; 91(1):44–47. PMID: 464453.
Article10. Shojaei-Far Z, Razi F, Bandarian F, Rambod C, Qorbani M. A detailed comparison of morning and random urine specimen levels with 24 hour urinary excretion levels of seven biochemical parameters with a proposed formula. Ann Clin Lab Sci. 2017; 47(2):201–207. PMID: 28442523.11. Rodby RA, Rohde RD, Sharon Z, Pohl MA, Bain RP, Lewis EJ, et al. The urine protein to creatinine ratio as a predictor of 24-hour urine protein excretion in type 1 diabetic patients with nephropathy. Am J Kidney Dis. 1995; 26(6):904–909. PMID: 7503064.
Article12. Ruggenenti P, Gaspari F, Perna A, Remuzzi G. Cross sectional longitudinal study of spot morning urine protein:creatinine ratio, 24 hour urine protein excretion rate, glomerular filtration rate, and end stage renal failure in chronic renal disease in patients without diabetes. BMJ. 1998; 316(7130):504–509. PMID: 9501711.
Article13. Inker LA, Schmid CH, Tighiouart H, Eckfeldt JH, Feldman HI, Greene T, et al. Estimating glomerular filtration rate from serum creatinine and cystatin C. N Engl J Med. 2012; 367(1):20–29. PMID: 22762315.
Article14. Rees F, Hui M, Doherty M. Optimizing current treatment of gout. Nat Rev Rheumatol. 2014; 10(5):271–283. PMID: 24614592.
Article15. So A, Thorens B. Uric acid transport and disease. J Clin Invest. 2010; 120(6):1791–1799. PMID: 20516647.
Article16. Maesaka JK, Fishbane S. Regulation of renal urate excretion: a critical review. Am J Kidney Dis. 1998; 32(6):917–933. PMID: 9856507.
Article17. Enomoto A, Kimura H, Chairoungdua A, Shigeta Y, Jutabha P, Cha SH, et al. Molecular identification of a renal urate anion exchanger that regulates blood urate levels. Nature. 2002; 417(6887):447–452. PMID: 12024214.18. Miyazaki H, Sekine T, Endou H. The multispecific organic anion transporter family: properties and pharmacological significance. Trends Pharmacol Sci. 2004; 25(12):654–662. PMID: 15530644.
Article19. Hamada T, Ichida K, Hosoyamada M, Mizuta E, Yanagihara K, Sonoyama K, et al. Uricosuric action of losartan via the inhibition of urate transporter 1 (URAT 1) in hypertensive patients. Am J Hypertens. 2008; 21(10):1157–1162. PMID: 18670416.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Study on Effect of Benzbromarone in the Patients with Gout
- Management of Complicated Gout
- Updates in the management of gouty arthritis
- Prevention of Comorbidity and Acute Attack of Gout by Uric Acid Lowering Therapy
- The Effect of Low Dose Aspirin on Serum and Urinary Uric Acid Level in Gouty Arthritis Patients
