Pediatric liver transplantation with hyperreduced left lateral segment graft
- Affiliations
-
- 1Departments of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- 2Departments of Pediatrics, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- KMID: 2508860
- DOI: http://doi.org/10.14701/ahbps.2020.24.4.503
Abstract
- Backgrounds/Aims
To prevent large-for-size graft-related complications in small infant patients, the size of a left lateral segment (LLS) graft can be reduced to be a hyperreduced LLS (HRLLS) graft.
Methods
This study was intended to describe the detailed techniques for harvesting and implanting HRLLS grafts developed in a high-volume liver transplantation (LT) center.
Results
The mean recipient age was 4.0±1.7 months (range: 3-6) and body weight was 5.3±1.4 kg (range: 4.1-6.9). Primary diagnoses of the recipients were progressive familial intrahepatic cholestasis in 2 and biliary atresia in 1. The types of LT were living donor LT in 1 and split deceased donor LT in 2. Non-anatomical size reduction was performed to the transected LLS grafts. The mean weight of the HRLLS grafts was 191.7±62.1 g (range: 120-230) and graft-recipient weight ratio was 3.75±1.57% (range: 2.45-5.49). Widening venoplasty was applied to the graft left hepatic vein outflow orifice. Vein homograft interposition was used in a case with portal vein hypoplasia. Types of the abdomen wound closure were one case of primary repair, one of two-staged closure with a mesh, and one of three-staged repair with a silo and a mesh. All three patients recovered uneventfully from the LT operation and are doing well to date for more than 6 years after transplantation.
Conclusions
Making a HRLLS graft through non-anatomical resection during living donor LT and split deceased donor LT can be a useful option for treating small infant patients.
Keyword
Figure
-

Fig. 1 Computed tomography scans showing the left lateral segment appearing to be a flat fish (A) and puffy fish (B).

Fig. 2 Computed tomography scans showing the graft thickness-to-anteroposterior diameter in the recipient’s abdominal cavity ratio.

Fig. 3 Illustration of the extent of non-anatomic hepatic resection to make a hyperreduced left lateral segment graft.
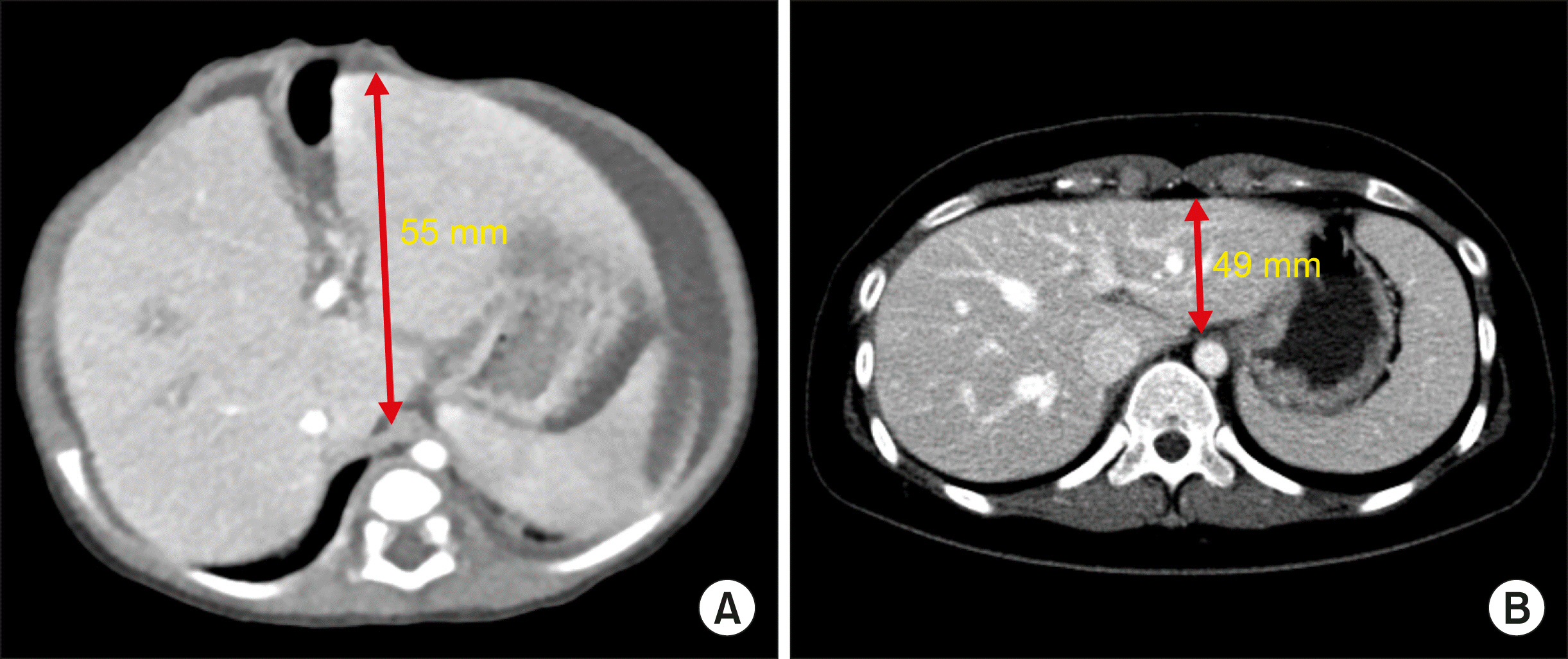
Fig. 4 Computed tomography scans showing the graft thickness (A)-to-anteroposterior diameter in the recipient’s abdominal cavity (B) ratio in Case No. 1. The graft thickness ratio was 0.89.

Fig. 5 Intraoperative photographs showing the size of abdomen (A) and native liver (B) in Case No. 1.

Fig. 6 Intraoperative photographs showing the surgical procedures for making a hyperreduced left lateral segment graft in Case No. 1. (A) The left hepatic artery and portal vein were isolated and hepatic parenchyma was transected. (B and C) The size of the left lateral segment graft was measured with a paper ruler. (D) Test parenchymal clamping was attempted. (E) The lines for size reduction were drawn on the liver surface. (F and G) The peripheral parts of the segment II and III were resected. (H) Some liver parenchyma was resected from the graft.
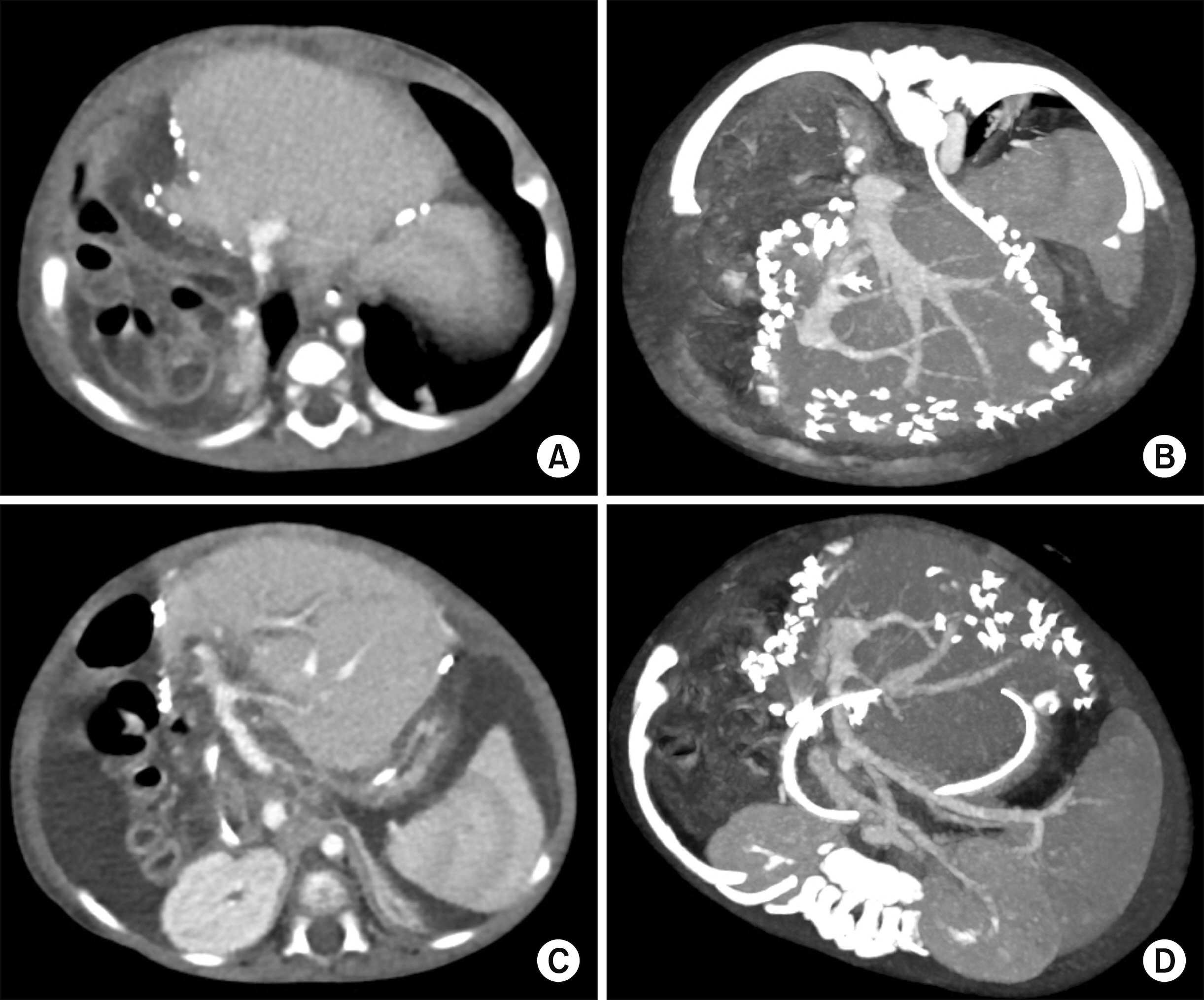
Fig. 7 Computed tomography scan taken four days after transplantation in the Case No. 1. The configurations of the graft left hepatic vein (A and B) and portal vein (C and D) reconstruction were smoothly streamlined.

Fig. 8 Computed tomography of the recipient at the age of 2 months (A) and gross photograph of the resected recipient’s liver (B) in Case No. 2.

Fig. 9 Intraoperative photographs showing the surgical procedures for making a split hyperreduced left lateral segment graft in Case No. 2. (A) The lines for liver splitting and size reduction were drawn on the liver surface. (B) The liver was split and size was also reduced. (C) The whole split liver was harvested. (D) An unification venoplasty was performed after septotomy and excision of the intervening hepatic parenchyma. (E) The hyperreduced liver graft was implanted. (F) The protruded liver graft was covered by a silo.
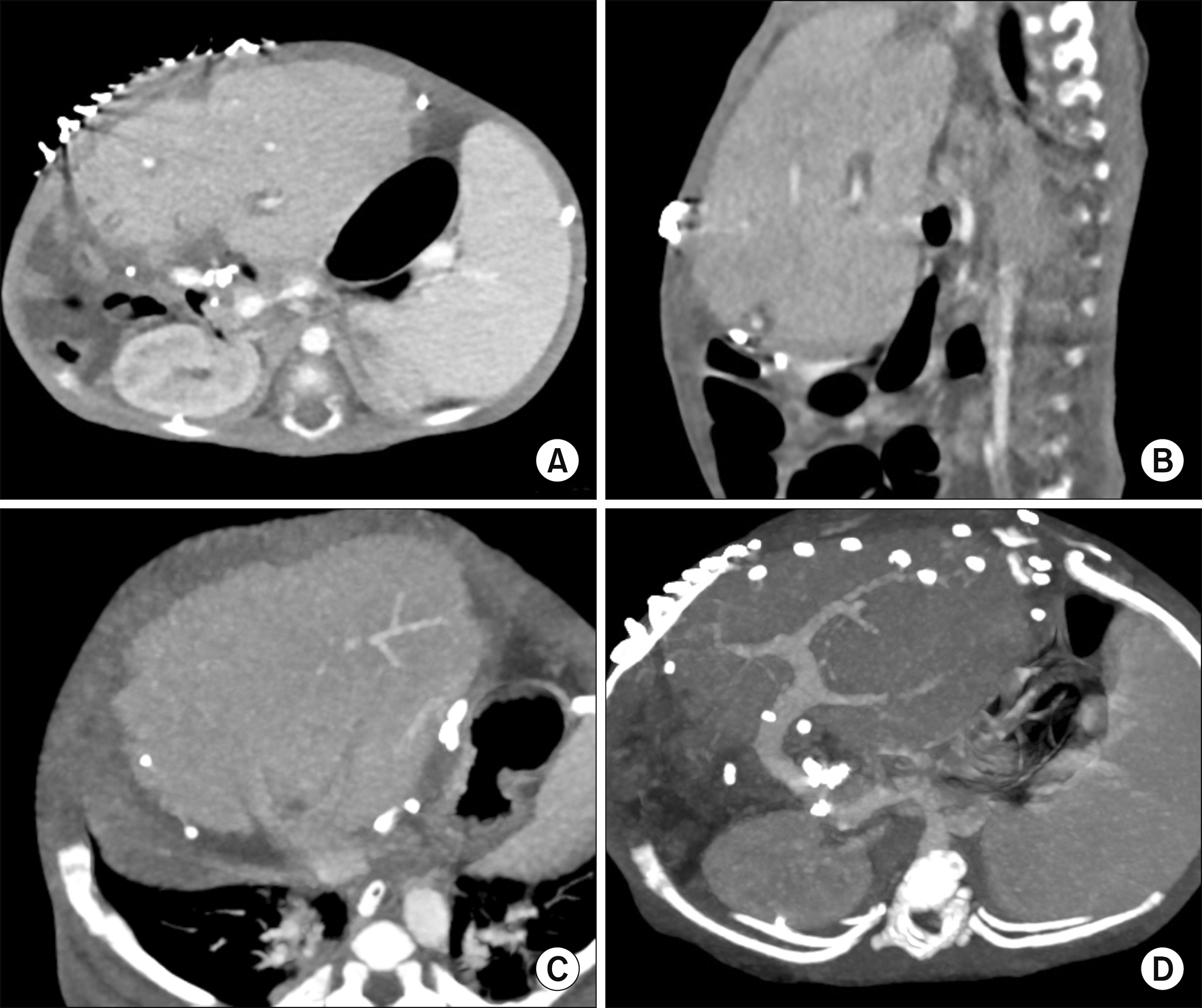
Fig. 10 Computed tomography scan taken 14 days after transplantation in Case No. 2. The abdominal wall was closed completely (A and B), and the graft hepatic vein (C) and portal vein (D) reconstructions were uneventful.
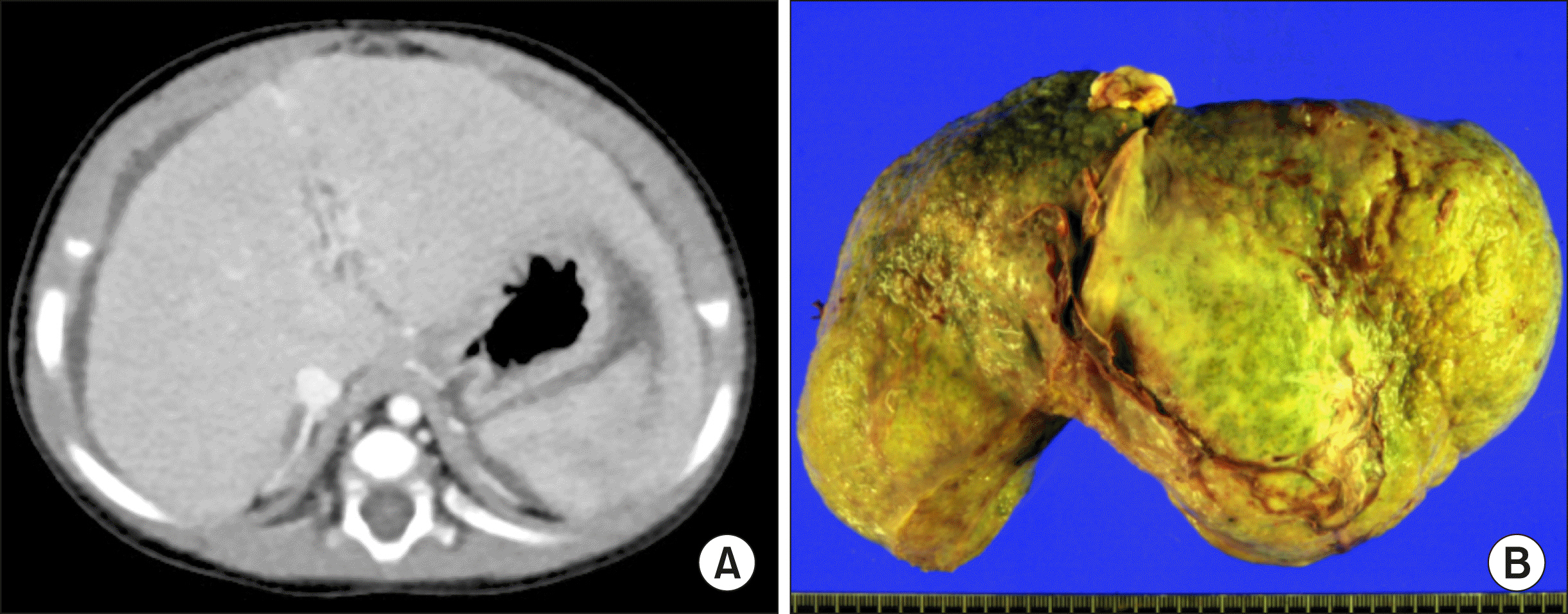
Fig. 11 Computed tomography of the recipient at the age of 5 months (A) and gross photograph of the resected recipient’s liver (B) in Case No. 3.

Fig. 12 Intraoperative photographs showing the surgical procedures for implantation of a split hyperreduced left lateral segment graft in Case No. 3. (A and B) The reduced graft was harvested. (C) The recipient’s portal vein was hypoplastic. (D) Recipient hepatectomy was performed. (E and F) The recipient’s portal vein was replaced with an external iliac vein homograft and portal vein reconstruction was performed. (G and H) The reduced graft was implanted, but it was too large to be accommodated within the abdomen, so the abdominal wound was temporarily closed with a xenograft patch.
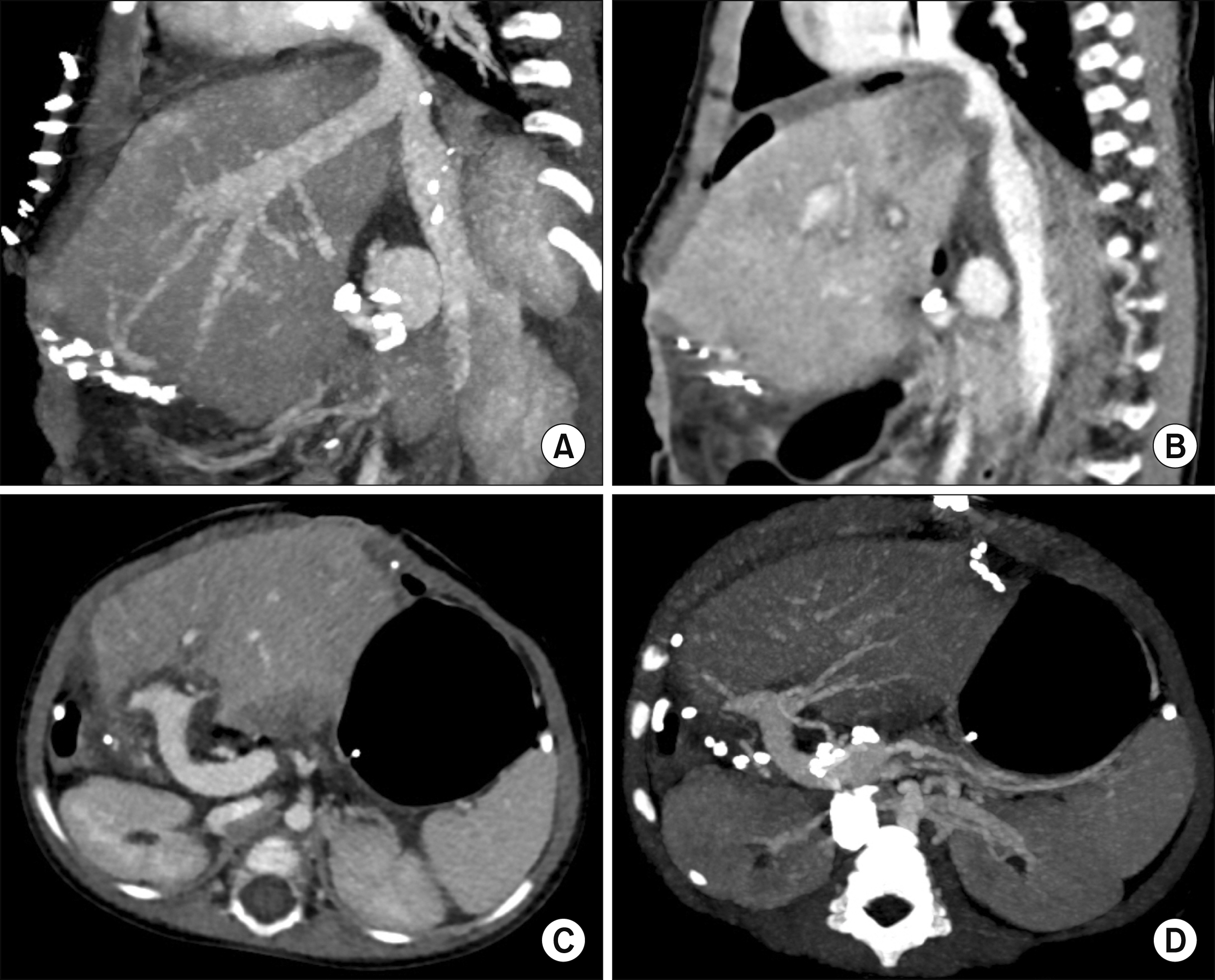
Fig. 13 Computed tomography scan taken at 5 days after transplantation in Case No. 3. The abdominal wall was temporarily closed with a thin patch (A and B), and the graft hepatic vein (A and B) and portal vein (C and D) reconstructions were uneventful.
Cited by 4 articles
-
Third retransplantation using a whole liver graft for late graft failure from hepatic vein stent stenosis in a pediatric patient who underwent split liver retransplantation
Jung-Man Namgoong, Shin Hwang, Young-In Yoon, Yong-Pil Cho, Woo-Hyoung Kang, Yong Jae Kwon, Hyunhee Kwon, Sang Hoon Kim, Kyung Mo Kim, Seak Hee Oh
Ann Hepatobiliary Pancreat Surg. 2021;25(2):299-306. doi: 10.14701/ahbps.2021.25.2.299.Dextroplantation of a reduced left lateral section graft in an infant undergoing living donor liver transplantation
Jung-Man Namgoong, Shin Hwang, Gil-Chun Park, Kyung Mo Kim, Seak Hee Oh, Hyunhee Kwon, Yong Jae Kwon
Ann Hepatobiliary Pancreat Surg. 2021;25(3):414-418. doi: 10.14701/ahbps.2021.25.3.414.Liver transplantation in pediatric patients with progressive familial intrahepatic cholestasis: Single center experience of seven cases
Jung-Man Namgoong, Shin Hwang, Hyunhee Kwon, Suhyeon Ha, Kyung Mo Kim, Seak Hee Oh, Seung-Mo Hong
Ann Hepatobiliary Pancreat Surg. 2022;26(1):69-75. doi: 10.14701/ahbps.21-114.Living donor liver transplantation with hyperreduced segment II monosegment graft for an infant weighing 3 kilograms
Jung-Man Namgoong, Gil-Chun Park, Shin Hwang, Sang-Hoon Kim, Suhyeon Ha, Kyung Mo Kim, Seak Hee Oh
Ann Liver Transplant. 2023;3(1):50-56. doi: 10.52604/alt.23.0001.
Reference
-
1. Kanazawa H, Sakamoto S, Fukuda A, Uchida H, Hamano I, Shigeta T, et al. 2013; Living-donor liver transplantation with hyperreduced left lateral segment grafts: a single-center experience. Transplantation. 95:750–754. DOI: 10.1097/TP.0b013e31827a93b4. PMID: 23503505.2. Shehata MR, Yagi S, Okamura Y, Iida T, Hori T, Yoshizawa A, et al. 2012; Pediatric liver transplantation using reduced and hyper-reduced left lateral segment grafts: a 10-year single-center experience. Am J Transplant. 12:3406–3413. DOI: 10.1111/j.1600-6143.2012.04268.x. PMID: 22994696.
Article3. Ardiles V, Ciardullo MA, D'Agostino D, Pekolj J, Mattera FJ, Boldrini GH, et al. 2013; Transplantation with hyper-reduced liver grafts in children under 10 kg of weight. Langenbecks Arch Surg. 398:79–85. DOI: 10.1007/s00423-012-1020-y. PMID: 23093088.4. Thomas N, Thomas G, Verran D, Stormon M, O'Loughlin E, Shun A. 2010; Liver transplantation in children with hyper-reduced grafts - a single-center experience. Pediatr Transplant. 14:426–430. DOI: 10.1111/j.1399-3046.2010.01294.x. PMID: 20214746.
Article5. Yamada N, Sanada Y, Hirata Y, Okada N, Wakiya T, Ihara Y, et al. 2015; Selection of living donor liver grafts for patients weighing 6kg or less. Liver Transpl. 21:233–238. DOI: 10.1002/lt.24048. PMID: 25422258.
Article6. Sakuma Y, Sasanuma H, Miki A, Shimizu A, Sata N, Yasuda Y, et al. 2016; Living-donor liver transplantation using segment 2 monosegment graft: a single-center experience. Transplant Proc. 48:1110–1114. DOI: 10.1016/j.transproceed.2015.12.119. PMID: 27320568.
Article7. Hong SK, Suh KS, Kim HS, Yoon KC, Ahn SW, Kim H, et al. 2018; Pediatric living donor liver transplantation using a monosegment procured by Pure 3D laparoscopic left lateral sectionectomy and in situ reduction. J Gastrointest Surg. 22:1135–1136. DOI: 10.1007/s11605-018-3705-1. PMID: 29435902.
Article8. Srinivasan P, Vilca-Melendez H, Muiesan P, Prachalias A, Heaton ND, Rela M. 1999; Liver transplantation with monosegments. Surgery. 126:10–12. DOI: 10.1067/msy.1999.98686. PMID: 10418586.
Article9. Lee S, Lee SK. 2013; Pediatric liver transplantation. J Korean Assoc Pediatr Surg. 19:14–21. DOI: 10.13029/jkaps.2013.19.1.14. PMID: 28502445.
Article10. Sakamoto S, Kanazawa H, Shigeta T, Uchida H, Sasaki K, Hamano I, et al. 2014; Technical considerations of living donor hepatectomy of segment 2 grafts for infants. Surgery. 156:1232–1237. DOI: 10.1016/j.surg.2014.05.003. PMID: 24909347.
Article11. Hwang S, Kim DY, Ahn CS, Moon DB, Kim KM, Park GC, et al. 2013; Computational simulation-based vessel interposition reconstruction technique for portal vein hypoplasia in pediatric liver transplantation. Transplant Proc. 45:255–258. DOI: 10.1016/j.transproceed.2012.05.090. PMID: 23375311.
Article12. Kiuchi T, Kasahara M, Uryuhara K, Inomata Y, Uemoto S, Asonuma K, et al. 1999; Impact of graft size mismatching on graft prognosis in liver transplantation from living donors. Transplantation. 67:321–327. DOI: 10.1097/00007890-199901270-00024. PMID: 10075602.13. Kasahara M, Fukuda A, Yokoyama S, Sato S, Tanaka H, Kuroda T, et al. 2008; Living donor liver transplantation with hyperreduced left lateral segments. J Pediatr Surg. 43:1575–1578. DOI: 10.1016/j.jpedsurg.2008.02.056. PMID: 18675660.
Article14. Vanatta JM, Esquivel CO. 2007; Status of liver transplantation in infants < 5 kg. Pediatr Transplant. 11:5–9. DOI: 10.1111/j.1399-3046.2006.00627.x. PMID: 17328158.15. Raices M, Czerwonko ME, Ardiles V, Boldrini G, D'Agostino D, Marcó Del Pont J, et al. 2019; Short- and long-term outcomes after live-donor transplantation with hyper-reduced liver grafts in low-weight pediatric recipients. J Gastrointest Surg. 23:2411–2420. DOI: 10.1007/s11605-019-04188-y. PMID: 30887299.
Article16. Hwang S, Kim KH, Kim DY, Kim KM, Ahn CS, Moon DB, et al. 2013; Anomalous hepatic vein anatomy of left lateral section grafts and customized unification venoplasty for pediatric living donor liver transplantation. Liver Transpl. 19:184–190. DOI: 10.1002/lt.23557. PMID: 23045153.
Article17. Namgoong JM, Hwang S, Park GC, Kwon H, Kwon YJ, Kim SH. 2020; Graft outflow vein unification venoplasty with superficial left hepatic vein branch in pediatric living donor liver transplantation using a left lateral section graft. Ann Hepatobiliary Pancreat Surg. 24:326–332. DOI: 10.14701/ahbps.2020.24.3.326. PMID: 32843600. PMCID: PMC7452796.
Article18. Kidd JN Jr, Jackson RJ, Smith SD, Wagner CW. 2003; Evolution of staged versus primary closure of gastroschisis. Ann Surg. 237:759–764. discussion 764-765. DOI: 10.1097/01.SLA.0000071568.95915.DC. PMID: 12796571. PMCID: PMC1514688.
Article19. Kwon H, Kwon H, Hong JP, Han Y, Park H, Song GW, et al. 2015; Use of cryopreserved cadaveric arterial allograft as a vascular conduit for peripheral arterial graft infection. Ann Surg Treat Res. 89:51–54. DOI: 10.4174/astr.2015.89.1.51. PMID: 26131446. PMCID: PMC4481033.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pediatric split liver transplantation using a hyperreduced left lateral segment graft in an infant weighing 4 kg
- Living donor liver transplantation with hyperreduced segment II monosegment graft for an infant weighing 3 kilograms
- Left at right heterotopic implantation of left liver graft in adult-to-adult living donor liver transplantation: the technical concern for decision-making
- Pediatric liver transplantation with hyperreduced left lateral segment graft
- Tailored techniques of graft outflow vein reconstruction in pediatric liver transplantation at Asan Medical Center
