Endocrinol Metab.
2020 Sep;35(3):562-570. 10.3803/EnM.2020.659.
Effects of Systemic Glucocorticoid Use on Fracture Risk: A Population-Based Study
- Affiliations
-
- 1Inhu-Chongno Pharmacy, Jeonju, Korea
- 2Department of Pharmacy, Mediplex Sejong Hospital, Incheon, Korea
- 3College of Pharmacy and Gachon Institute of Pharmaceutical Sciences, Gachon University, Incheon, Korea
- 4Department of Orthopaedic Surgery, Chung-Ang University College of Medicine, Seoul, Korea
- 5Department of Orthopaedic Surgery, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea
- 6Department of Orthopaedic Surgery, Seoul National University Bundang Hospital, Seongnam, Korea
- 7Department of Internal Medicine, Gangneung Asan Hospital, University of Ulsan College of Medicine, Gangneung, Korea
- KMID: 2508005
- DOI: http://doi.org/10.3803/EnM.2020.659
Abstract
- Background
Long-term glucocorticoid use increases fracture risk by reducing bone mass. This study evaluated the relationship between hip and vertebral fractures and the total amount of systematic glucocorticoid use.
Methods
We randomly selected 1,896,159 people aged 20 to 100 years who participated in the National Health Checkup program in 2006. The amount of glucocorticoids prescribed was calculated based on the defined daily dose (DDD). The total DDD was obtained by adding oral and parenteral glucocorticoids for 6 months from the index date. Subjects were categorized into four groups according to total glucocorticoid DDDs: non-users (DDDs=0), low users (0< DDDs ≤45), intermediate users (45< DDDs ≤90), and high users (90< DDDs). We followed them for 2 years. A multivariate Cox proportional hazard model was used to evaluate the effects of the total amount of glucocorticoid use on hip and vertebral fractures.
Results
Higher glucocorticoid use was associated with a higher risk of vertebral fracture. Relative to non-users, the vertebral fracture risk was 1.39 times higher in the low-user group, 1.94 times higher in the intermediate-user group, and 2.43 times higher in the highuser group. The risk of hip fracture was 1.72 times higher in intermediate users and 3.28 times higher in high users than in non-users.
Conclusion
As the amount of glucocorticoid use for 6 months increased, the risk of hip and vertebral fractures became higher. In order to prevent fractures, it is necessary for doctors to evaluate the total amount of glucocorticoid prescribed to the patient and to provide appropriate treatment.
Keyword
Figure
-

Fig. 1 Selection of study subjects. GC, glucocorticoid; BMI, body mass index.
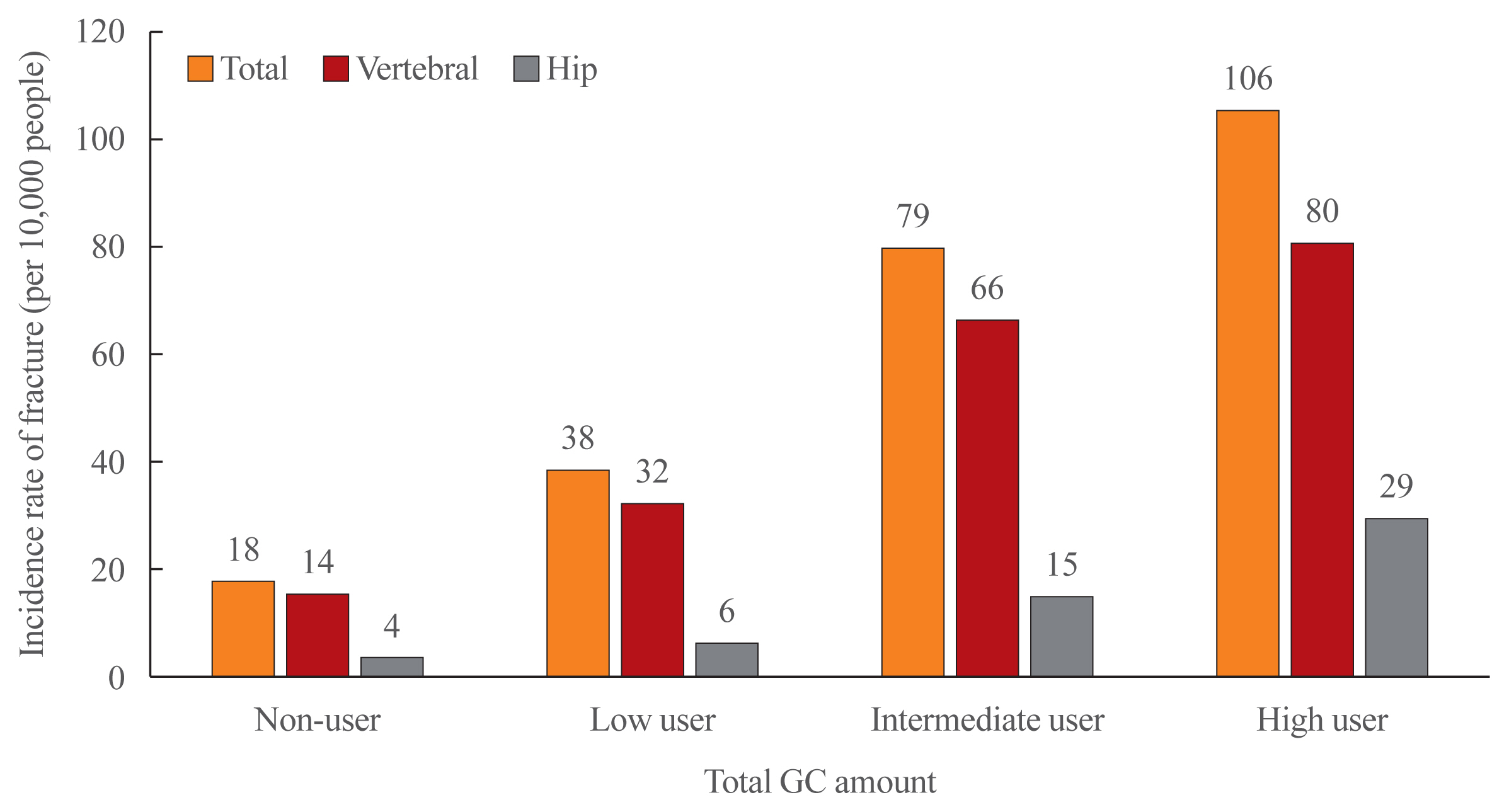
Fig. 2 Unadjusted incidence rate of vertebral and hip fracture by glucocorticoid (GC) amount the relationship between glucocorticoid exposure and fracture risk.
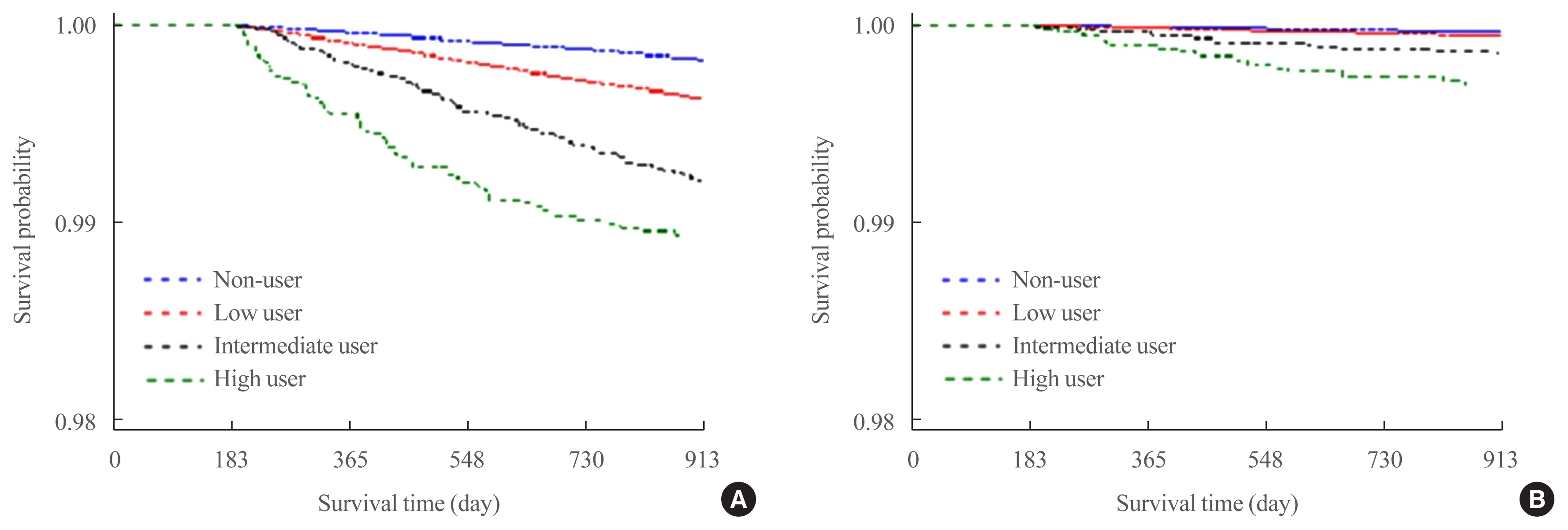
Fig. 3 Survival distribution function estimates for fracture. (A) Vertebral fracture. (B) Hip fracture.
Cited by 1 articles
-
Why Do We Need Proactive Management for Fracture Prevention in Long-Term Glucocorticoid Users?
Han Seok Choi
Endocrinol Metab. 2020;35(3):549-551. doi: 10.3803/EnM.2020.308.
Reference
-
1. Saag KG, Koehnke R, Caldwell JR, Brasington R, Burmeister LF, Zimmerman B, et al. Low dose long-term corticosteroid therapy in rheumatoid arthritis: an analysis of serious adverse events. Am J Med. 1994; 96:115–23.
Article2. Lane NE, Lukert B. The science and therapy of glucocorticoid-induced bone loss. Endocrinol Metab Clin North Am. 1998; 27:465–83.
Article3. Buckley L, Humphrey MB. Glucocorticoid-induced osteoporosis. N Engl J Med. 2018; 379:2547–56.
Article4. Panday K, Gona A, Humphrey MB. Medication-induced osteoporosis: screening and treatment strategies. Ther Adv Musculoskelet Dis. 2014; 6:185–202.
Article5. LoCascio V, Bonucci E, Imbimbo B, Ballanti P, Adami S, Milani S, et al. Bone loss in response to long-term glucocorticoid therapy. Bone Miner. 1990; 8:39–51.
Article6. Van Staa TP, Leufkens HG, Abenhaim L, Zhang B, Cooper C. Use of oral corticosteroids and risk of fractures. June, 2000. J Bone Miner Res. 2005; 20:1487–94.7. Fardet L, Petersen I, Nazareth I. Prevalence of long-term oral glucocorticoid prescriptions in the UK over the past 20 years. Rheumatology (Oxford). 2011; 50:1982–90.
Article8. Overman RA, Yeh JY, Deal CL. Prevalence of oral glucocorticoid usage in the United States: a general population perspective. Arthritis Care Res (Hoboken). 2013; 65:294–8.
Article9. Kim HY, Jang EJ, Park B, Kim TY, Shin SA, Ha YC, et al. Development of a Korean Fracture Risk Score (KFRS) for predicting osteoporotic fracture risk: analysis of data from the Korean National Health Insurance Service. PLoS One. 2016; 11:e0158918.
Article10. Kanis JA, Johansson H, Oden A, Johnell O, de Laet C, Melton LJ III, et al. A meta-analysis of prior corticosteroid use and fracture risk. J Bone Miner Res. 2004; 19:893–9.
Article11. Kanis JA, Johansson H, Oden A, McCloskey EV. Guidance for the adjustment of FRAX according to the dose of glucocorticoids. Osteoporos Int. 2011; 22:809–16.
Article12. De Vries F, Bracke M, Leufkens HG, Lammers JW, Cooper C, Van Staa TP. Fracture risk with intermittent high-dose oral glucocorticoid therapy. Arthritis Rheum. 2007; 56:208–14.
Article13. Mandel S, Schilling J, Peterson E, Rao DS, Sanders W. A retrospective analysis of vertebral body fractures following epidural steroid injections. J Bone Joint Surg Am. 2013; 95:961–4.
Article14. Sutter SA, Stein EM. The skeletal effects of inhaled glucocorticoids. Curr Osteoporos Rep. 2016; 14:106–13.
Article15. Choi JH, Kim GA, Park JH, Song GH, Park JW, Kim DY, et al. Generation of viable embryos and embryonic stem cell-like cells from cultured primary follicles in mice. Biol Reprod. 2011; 85:744–54.16. Lim S, Koo BK, Lee EJ, Park JH, Kim MH, Shin KH, et al. Incidence of hip fractures in Korea. J Bone Miner Metab. 2008; 26:400–5.
Article17. Lippuner K. Epidemiology of osteoporotic fractures in Switzerland. Rev Med Suisse. 2009; 5:1304–8.18. Park C, Ha YC, Jang S, Jang S, Yoon HK, Lee YK. The incidence and residual lifetime risk of osteoporosis-related fractures in Korea. J Bone Miner Metab. 2011; 29:744–51.
Article19. Balasubramanian A, Wade SW, Adler RA, Lin CJF, Maricic M, O’Malley CD, et al. Glucocorticoid exposure and fracture risk in patients with new-onset rheumatoid arthritis. Osteoporos Int. 2016; 27:3239–49.
Article20. Bultink IE, Harvey NC, Lalmohamed A, Cooper C, Lems WF, van Staa TP, et al. Elevated risk of clinical fractures and associated risk factors in patients with systemic lupus erythematosus versus matched controls: a population-based study in the United Kingdom. Osteoporos Int. 2014; 25:1275–83.
Article21. Oshagbemi OA, Burden AM, Shudofsky KN, Driessen JHM, Vestergaard P, Krings A, et al. Use of high-dose intermittent systemic glucocorticoids and the risk of fracture in patients with chronic obstructive pulmonary disease. Bone. 2018; 110:238–43.
Article22. Ioannidis G, Pallan S, Papaioannou A, Mulgund M, Rios L, Ma J, et al. Glucocorticoids predict 10-year fragility fracture risk in a population-based ambulatory cohort of men and women: Canadian Multicentre Osteoporosis Study (CaMos). Arch Osteoporos. 2014; 9:169.
Article23. van Staa TP, Leufkens HG, Abenhaim L, Zhang B, Cooper C. Oral corticosteroids and fracture risk: relationship to daily and cumulative doses. Rheumatology (Oxford). 2000; 39:1383–9.
Article24. Angeli A, Guglielmi G, Dovio A, Capelli G, de Feo D, Giannini S, et al. High prevalence of asymptomatic vertebral fractures in post-menopausal women receiving chronic glucocorticoid therapy: a cross-sectional outpatient study. Bone. 2006; 39:253–9.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Understanding of Glucocorticoid Induced Osteoporosis
- Management of glucocorticoid-related osteoporotic vertebral fracture
- Glucocorticoid-induced Osteoporosis
- Update on Glucocorticoid Induced Osteoporosis
- Prevalence of osteoporosis in patients with systemic lupus erythematosus: A multicenter comparative study of the World Health Organization and fracture risk assessment tool criteria
