The experience of infection prevention for coronavirus disease 2019 (COVID-19) during general anesthesia in an epidemic of COVID-19: including unexpected exposure case - Two cases report -
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Daegu Fatima Hospital, Daegu, Korea
- KMID: 2504904
- DOI: http://doi.org/10.17085/apm.20044
Abstract
- Background
Coronavirus disease 2019 (COVID-19) has been an epidemic in the Republic of Korea since the first patient who came in China was confirmed as having the disease on January 19, 2020. Therefore, surgery for COVID-19-related patients is expected to increase. Case: We experienced two cases of COVID-19-related patients who underwent surgery for femur fracture under general anesthesia. In one case, infection control to prevent transmission was achieved, while in the second case, healthcare workers were exposed to severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2).
Conclusions
In areas where there is COVID-19 epidemic, SARS-CoV-2 RT-PCR should be performed before surgery in patients with symptoms of respiratory infection such as fever, cough, and sputum, or for those in whom the possibility of COVID-19 cannot be completely excluded. Efforts should be made to prevent healthcare worker’s exposure and the contamination of the operating room.
Keyword
Figure
-
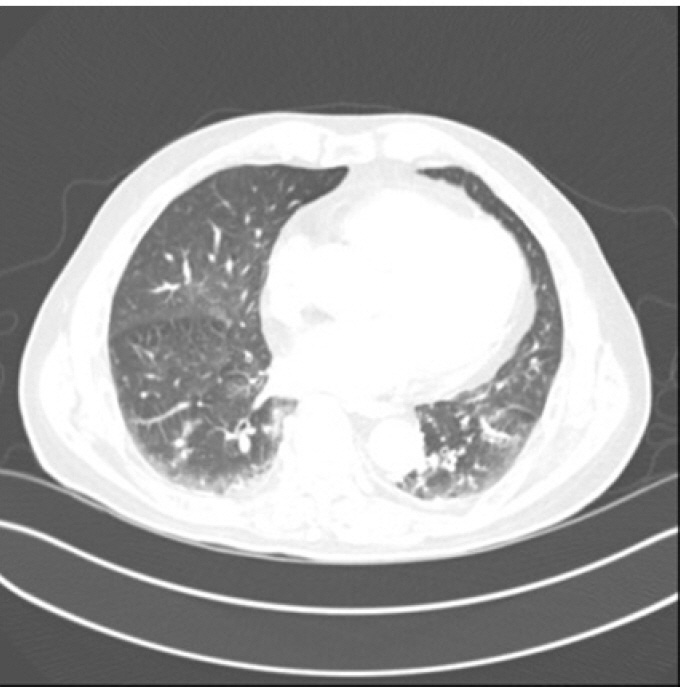
Fig. 1. Chest CT showed consolidations in both lower lung which were suspected as pneumonia. CT: computed tomography.
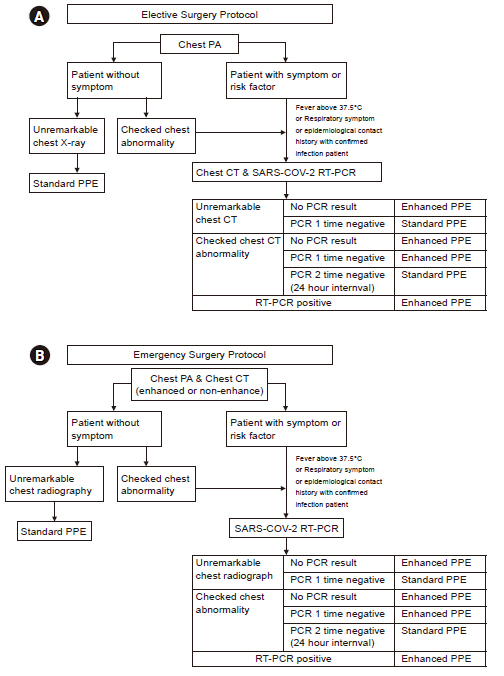
Fig. 2. (A) When planning elective surgery, Chest X-ray was performed first. If the possibility of SARS-CoV-2 infection could not be completely ruled out, chest CT and RT-PCR were also performed. (B) In the case of emergency surgery, chest CT was checked as well as chest X-ray in all patients. SARS-CoV-2 PCR was performed when abnormality in Chest CT was detected, patients had risk factors, or respiratory symptoms such as cough and sputum. RT-PCR: real-time polymerase chain reaction, PPE: personal protective equipment, SARS-CoV-2: severe acute respiratory syndrome coronavirus-2, COVID-19: coronavirus disease 2019, CT: computed tomography, PA: posteroanterior.
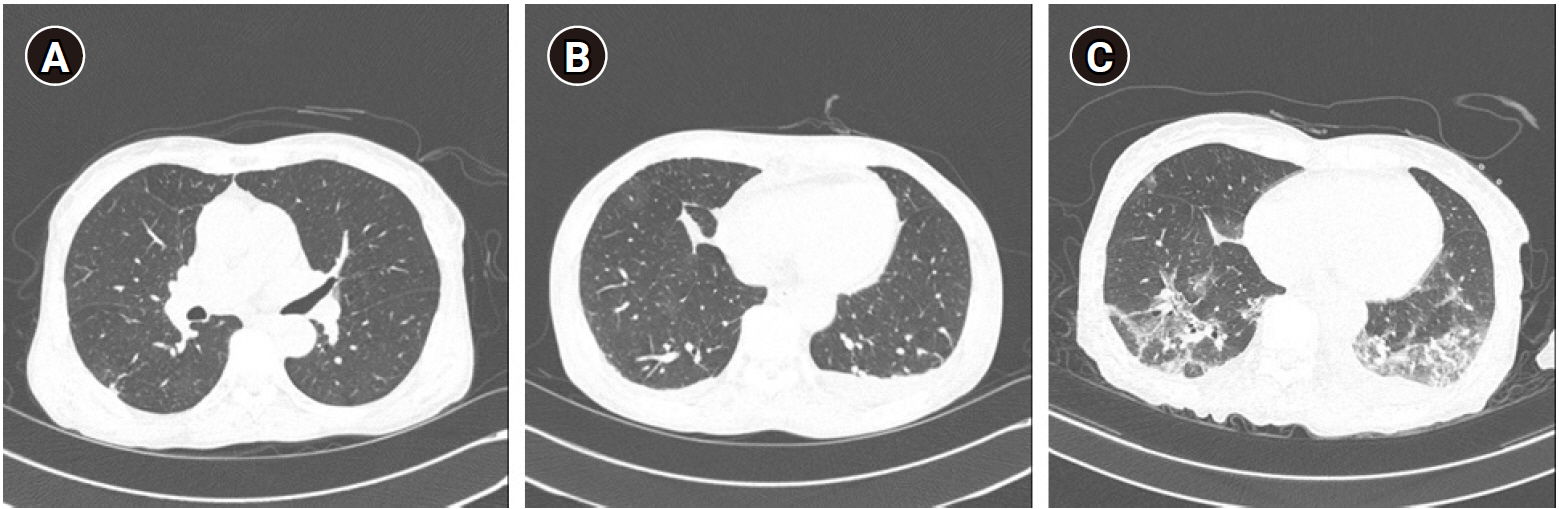
Fig. 3. (A) Chest CT showed no evidence of active infection and no change in the interval of old tuberculosis. (B) Chest CT showed increased bilateral pleural effusion and no interval change of GGA in the right lower lung. (C) Chest CT showed a multifocal patchy GGA lesion with interlobular septal thickening that appears to be a new suspected viral pneumonia. CT: computed tomography, GGA: ground-glass appearance.
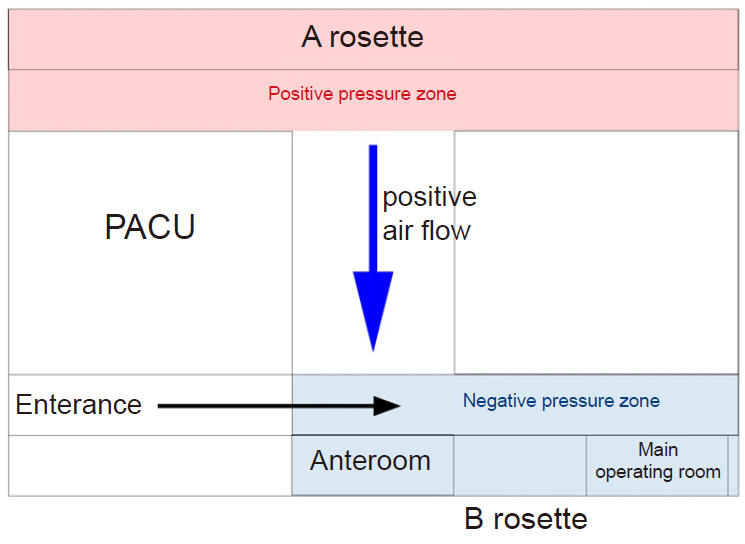
Fig. 4. This picture is a schematic diagram of our operating hall. We set up rosette A and rosette B. The rosette close to the entrance was set as a negative pressure zone. PACU: post-anesthesia care unit.
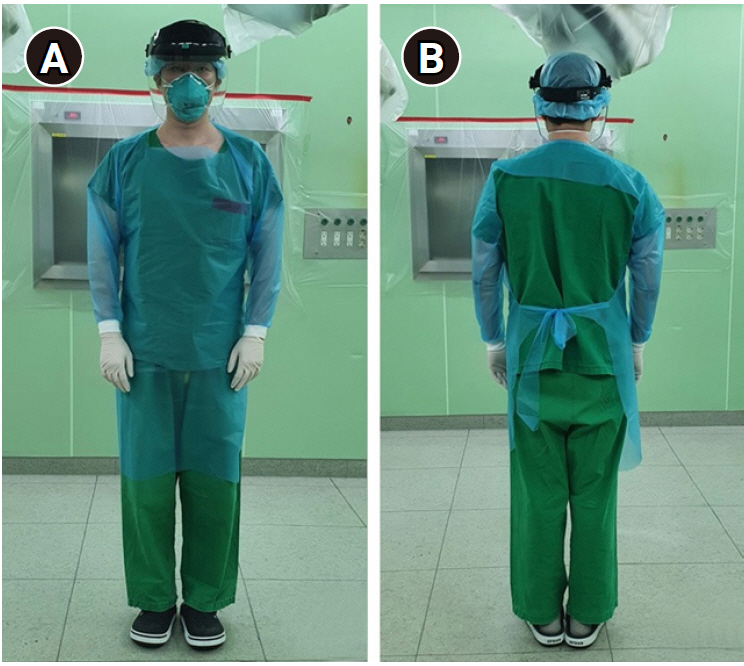
Fig. 5. Standard personal protective equipment in frontal view (A) and back view (B).

Fig. 6. Enhanced personal protective equipment in frontal view (A) and back view (B).
Reference
-
1. COVID-19 [serial on the Internet]. Cheongju: Korea Centers for Disease Control & Prevention [cited 2020 May 12]. Available from http://ncov.mohw.go.kr/.2. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020; 395:497–506.3. de Wit E, van Doremalen N, Falzarano D, Munster VJ. SARS and MERS: recent insights into emerging coronaviruses. Nat Rev Microbiol. 2016; 14:523–34.4. Chan JF, Yuan S, Kok KH, To KK, Chu H, Yang J, et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster. Lancet. 2020; 395:514–23.5. World Health Organization. Infection prevention and control during health care when COVID-19 is suspected [serial on the Internet]. 2020 Mar 19 [cited 2020 May 12]. Available from https://www.who.int/publications/i/item/infection-prevention-and-control-during-health-care-when-novel-coronavirus-(ncov)-infection-is-suspected-20200125.6. Tran K, Cimon K, Severn M, Pessoa-Silva CL, Conly J. Aerosol generating procedures and risk of transmission of acute respiratory infections to healthcare workers: a systematic review. PLoS One. 2012; 7:e35797.7. Park J, Yoo SY, Ko JH, Lee SM, Chung YJ, Lee JH, et al. Infection prevention measures for surgical procedures during a Middle East respiratory syndrome outbreak in a tertiary care hospital in South Korea. Sci Rep. 2020; 10:325.8. Wong HYF, Lam HYS, Fong AH, Leung ST, Chin TW, Lo CSY, et al. Frequency and distribution of chest radiographic findings in COVID-19 positive patients. Radiology. 2020; doi: 10.1148/radiol.2020201160. [Epub ahead of print].9. Xie X, Zhong Z, Zhao W, Zheng C, Wang F, Liu J. Chest CT for typical 2019-nCoV pneumonia: relationship to negative RT-PCR testing. Radiology. 2020; doi: 10.1148/radiol.2020200343. [Epub ahead of print].10. Hong KH, Lee SW, Kim TS, Huh HJ, Lee J, Kim SY, et al. Guidelines for laboratory diagnosis of coronavirus disease 2019 (COVID-19) in Korea. Ann Lab Med. 2020; 40:351–60.11. van Doremalen N, Bushmaker T, Morris DH, Holbrook MG, Gamble A, Williamson BN, et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N Engl J Med. 2020; 382:1564–7.12. Greenland JR, Michelow MD, Wang L, London MJ. COVID-19 infection: implications for perioperative and critical care physicians. Anesthesiology. 2020; 132:1346–61.13. Guan W, Ni Z, Hu Y, Liang W, Ou C, He J, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020; 382:1708–20.14. Li Q, Guan X, Wu P, Wang X, Zhou L, Tong Y, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med. 2020; 382:1199–207.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- COVID-19 and Fungal Infection
- Treatment for Immune Thrombocytopenia in Coronavirus Disease 2019 (COVID-19) Infection after COVID-19 Vaccination: A Case Report
- Updates on Coronavirus Disease 19 Vaccine and Its Clinical Application
- Stroke in a Young Age COVID-19 Patient: Vasculitis Feature and Changes in Cerebral Vessel Stenosis
- COVID-19 and Smell Loss
