Baha Attract Implantation Using a Small Incision: Initial Report of Surgical Technique and Surveillance
- Affiliations
-
- 1Department of Sculpture, Hongik University, Seoul, Korea
- 2Department of Fine Arts Education, Kyungnam University, Changwon, Korea
- 3Department of Speech Pathology and Audiology, Research Institute of Audiology and Speech Pathology, College of Natural Sciences, Hallym University, Chuncheon, Korea
- 4Department of Otorhinolaryngology, Yonsei University Wonju College of Medicine, Wonju, Korea
- KMID: 2501292
- DOI: http://doi.org/10.21053/ceo.2019.00381
Abstract
Objectives
. To determine the appropriate anatomical borders of implantation on the temporal bone in a cadaver study, and to develop a simplified surgical technique for Baha Attract implantation through a small incision along the hairline using anatomical evidence and a navigation system.
Methods
. In a cadaver study, 20 human adult dry skulls were used to find flat areas of the temporal bone for Baha Attract magnet implantation. Four borders of the “optimal surgical site” were defined: Asterion line, occipitomastoid suture line, sigmoid sinus line, and digastric groove line. In three patients, we implanted the Baha Attract according to the newly developed surgical procedure and validated the feasibility of this technique with a navigation system.
Results
. We identified the appropriate position of the implant on the temporal bone, suggesting a simplified surgical technique for Baha Attract with a small incision. We determined the spot of implantation, and the implants were inserted through a small surgical incision (<2.5 cm) under local anesthesia; the procedure lasted approximately 30 minutes.
Conclusion
. The optimal surgical site of the temporal bone is a safe and easily accessible location for implantation of the Baha Attract.
Keyword
Figure
-
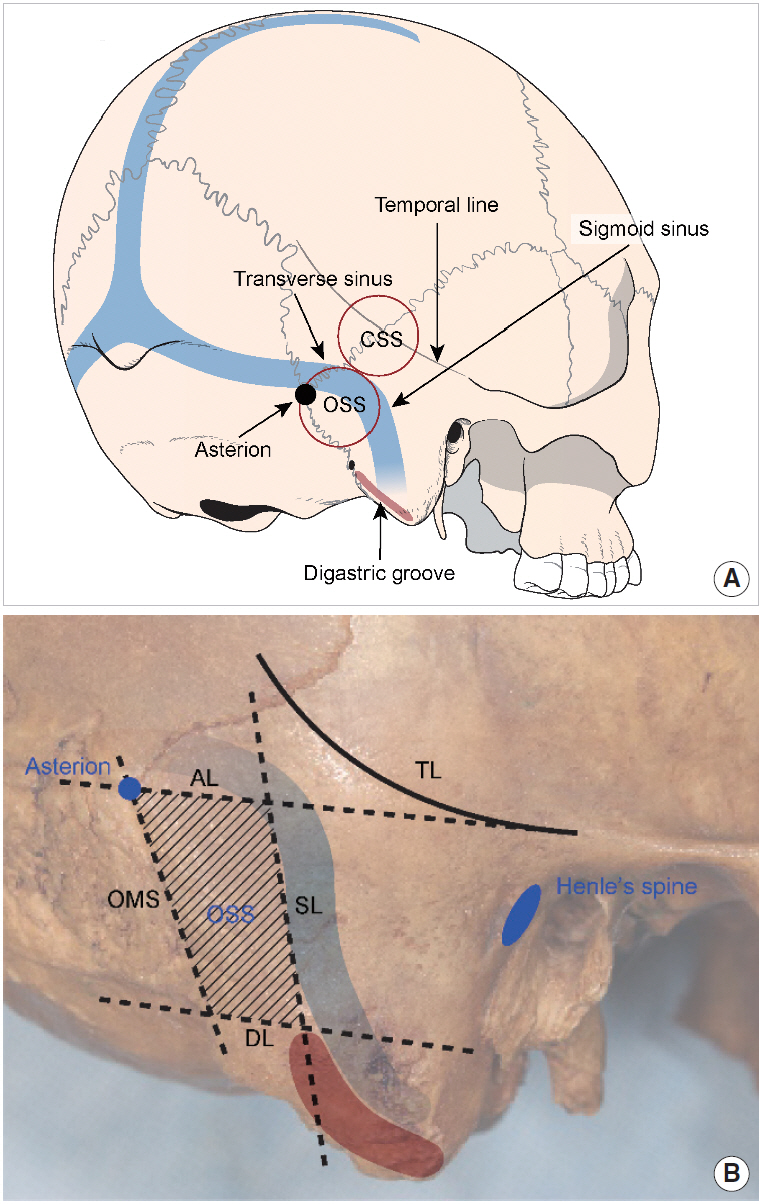
Fig. 1. (A) The anatomical distribution of the temporal bone shows that the optimal surgical site (OSS), with a relatively flat surface, is a better position for the Baha Attract implant. (B) The four borders of the OSS are the Asterion line (AL), sigmoid sinus line (SL), occipitomastoid suture line (OMS), and digastric groove line (DL). The average distances from the spine of Henle horizontally to the Asterion and to the Sigmoid sinus are necessary to determine the location of the implant during surgery. As the size of the implanted magnet is 27 mm, the area of the OSS should be sufficient. CSS, conventional surgical site; TL, temporal line.
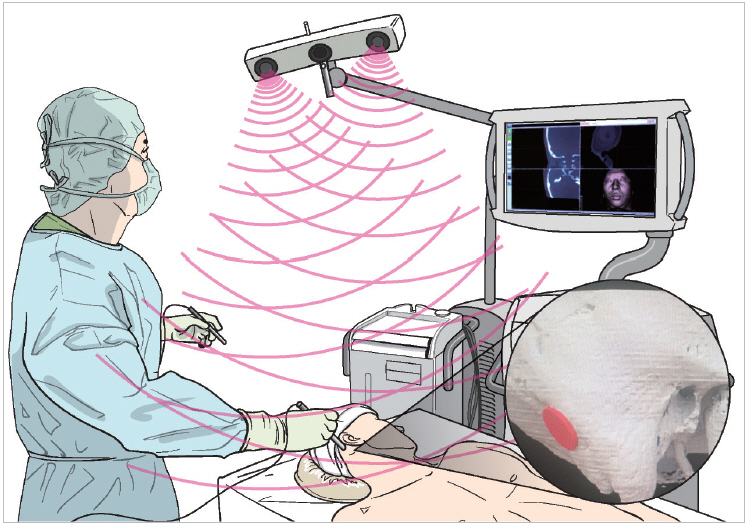
Fig. 2. The navigation system view during the implantation of Baha Attract. Just before the surgery, we marked the spot of the implant in the patient with the appropriate position measured in previous temporal bone computed tomography.
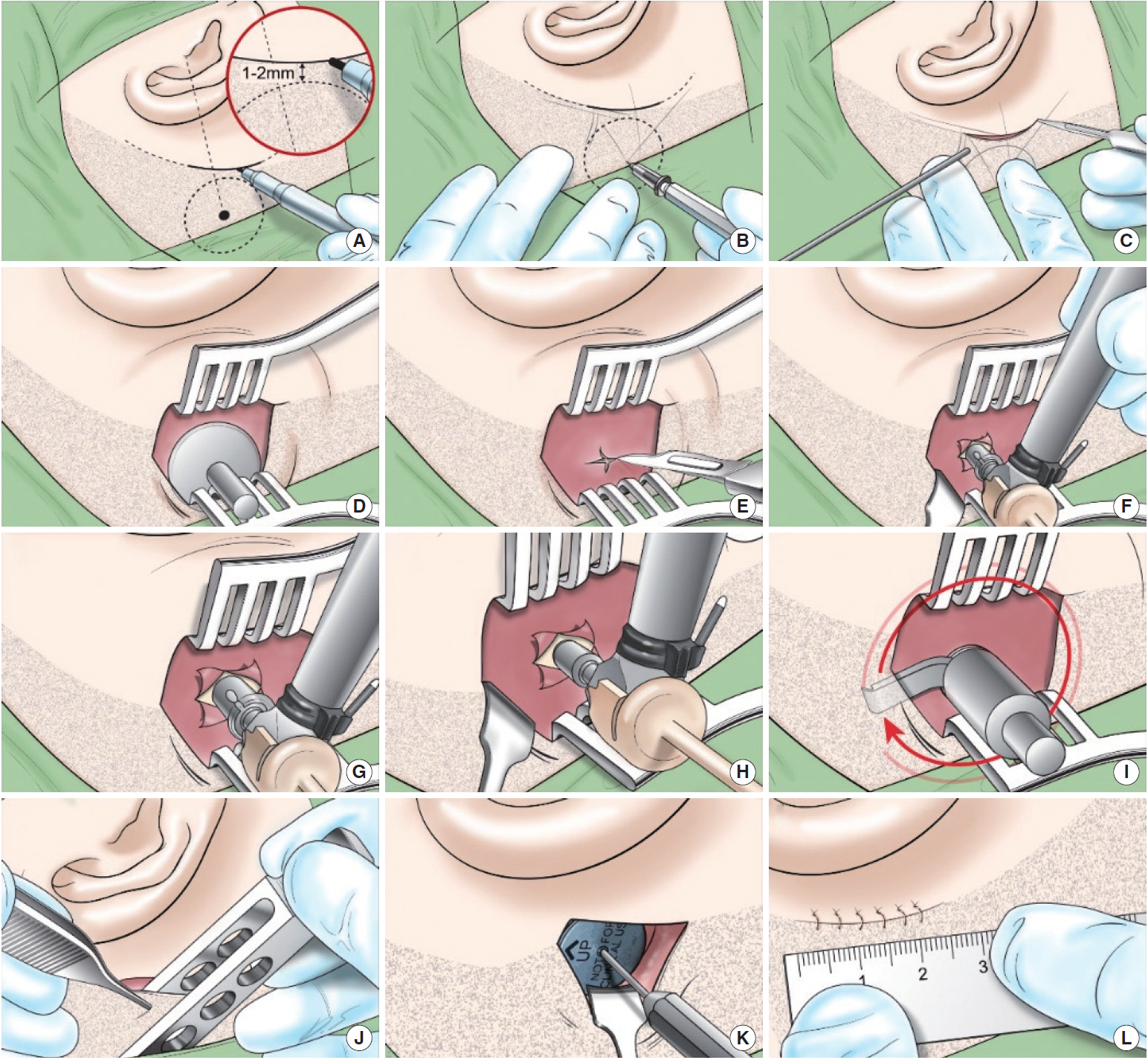
Fig. 3. The steps of the newly developed surgical procedure for implantation of the Baha Attract. (A) The small incision line along the patient’s hairline was marked. (B) The soft tissue thickness was measured with a thin needle. (C) An incision was made down to the periosteum. (D) The implant magnet template was placed on the periosteum. (E) A cruciate incision was made on the periosteum, and the periosteum was lifted. (F) The bone was drilled with a guide drill to a depth of 4 mm. (G) The hole was widened with the widening drill. (H) The implant was placed with a torque of 40–50 N-cm. (I) The bone bed indicator was used to confirm that the implant did not touch the bone or periosteum around the implant. (J) The thickness of the flap was evaluated with the soft tissue gauge, and should be 3–6 mm. If the skin flap was thicker than the reference point, the flap was thinned to 6 mm. (K) The implanted magnet was attached and screwed clockwise. (L) The skin was sutured to the periosteum over the implanted magnet. In the previous method provided by Cochlear Americas Corporation, a large C-shaped incision with a 150° angle across the hairline remained. Due to the large flap, additional steps were necessary to find a flat area of bone and to avoid the suture lines in the bone.
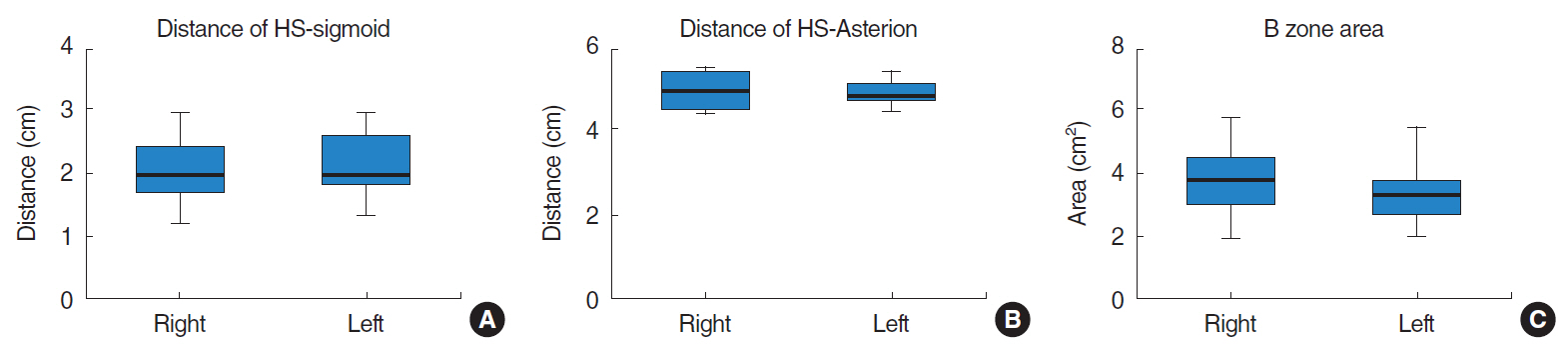
Fig. 4. Topographical distributions of the temporal bone. There was no difference between the right and left sides. (A) The distance from the spine of Henle (HS) to the sigmoid sinus (sigmoid) was 2.04±0.01 cm on the right side and 2.14±0.10 cm on the left side (P=0.499). (B) The distance from the HS to the Asterion was 5.05±0.09 cm on the right and 4.97±0.07 cm on the left (P=0.479). (C) The area of the optimal surgical site was 3.74±0.24 cm2 on the right and 3.37±0.18 cm2 on the left (P=0.225).

Fig. 5. The postoperative figures of the incision site. (A) and (C) show small incisions according to the hairlines of two patients 2 weeks after implantation. Patients in (B), (D), and (E) showed no scars in the postauricular area after 2 months. (F) The scar of a 63-year-old woman who received the implant through a large C-shaped incision, 6 months after implantation (white arrows).
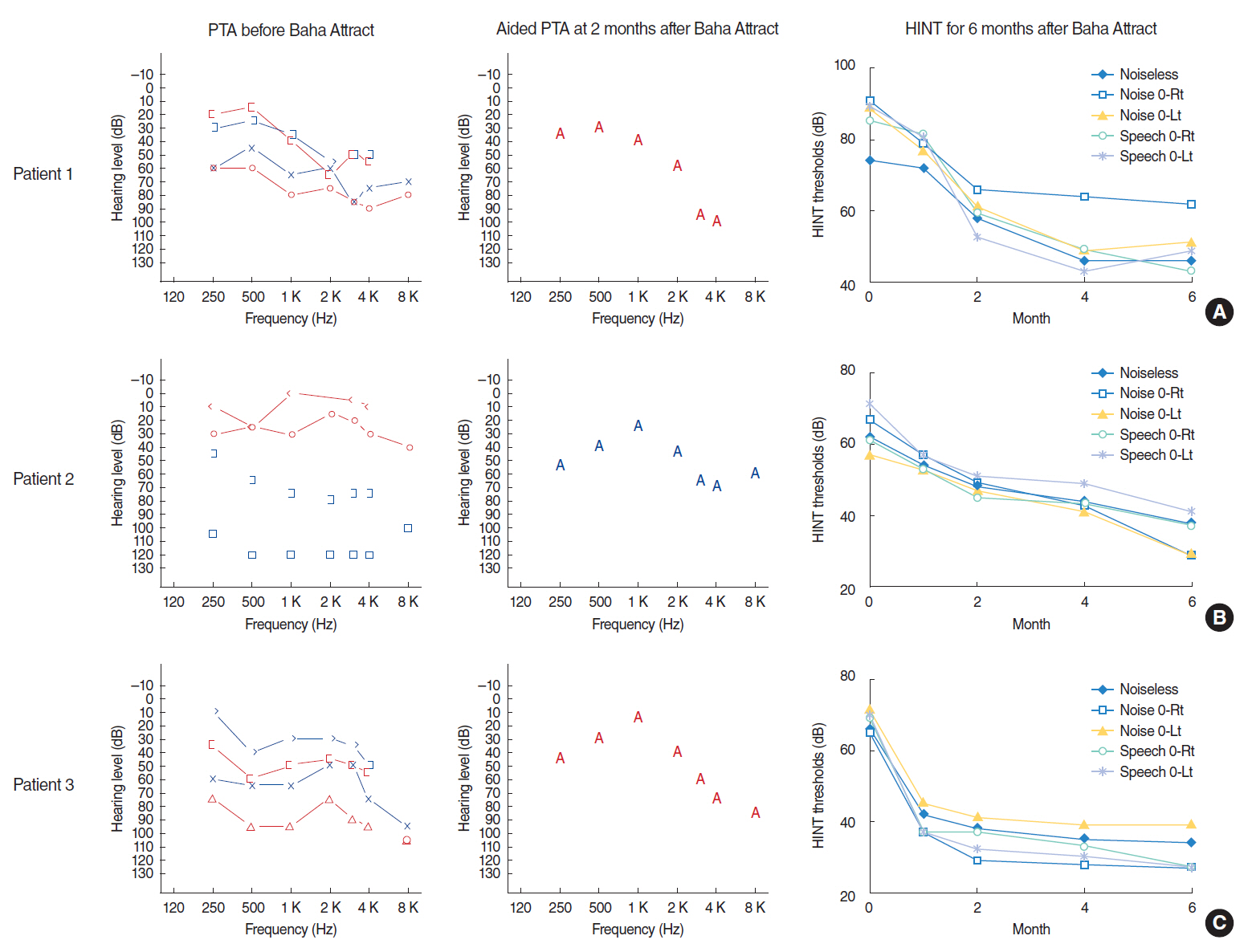
Fig. 6. Three patients who received the Baha Attract system using simplified surgery with the small incision; all scored well on the audiologic tests (sound field and Hearing in Noise Test [HINT]). Two patients with mixed hearing loss (A, C) as well as patient 2 (B), who had a type of sensorineural hearing loss, also recovered to approximately 40 dB on the surgical side. Compared with preoperative hearing (75, scaled out, and 90 dB), the hearing gains were excellent. The HINT results showed that initial improvement was rapid, and gradual improvement continued during the 6-month follow-up. PTA, pure tone audiometry; Rt, right; Lt, left.
Cited by 1 articles
-
Efficacy of Implantable Bone Conduction Hearing Aids in Single-Sided Deafness
Ji Hyeon Lee, Young Joon Seo
Korean J Otorhinolaryngol-Head Neck Surg. 2020;63(7):293-300. doi: 10.3342/kjorl-hns.2020.00514.
Reference
-
1. Clamp PJ, Briggs RJ. The Cochlear Baha 4 Attract System: design concepts, surgical technique and early clinical results. Expert Rev Med Devices. 2015; May. 12(3):223–30.2. Hakansson B, Tjellstrom A, Rosenhall U, Carlsson P. The bone-anchored hearing aid: principal design and a psychoacoustical evaluation. Acta Otolaryngol. 1985; Sep-Oct. 100(3-4):229–39.3. House JW, Kutz JW Jr. Bone-anchored hearing aids: incidence and management of postoperative complications. Otol Neurotol. 2007; Feb. 28(2):213–7.4. Kurz A, Flynn M, Caversaccio M, Kompis M. Speech understanding with a new implant technology: a comparative study with a new nonskin penetrating Baha system. Biomed Res Int. 2014; 2014:416205.
Article5. Iseri M, Orhan KS, Tuncer U, Kara A, Durgut M, Guldiken Y, et al. Transcutaneous bone-anchored hearing aids versus percutaneous ones: multicenter comparative clinical study. Otol Neurotol. 2015; Jun. 36(5):849–53.6. Siegert R. Partially implantable bone conduction hearing aids without a percutaneous abutment (Otomag): technique and preliminary clinical results. Adv Otorhinolaryngol. 2011; 71:41–6.
Article7. Siegert R, Kanderske J. A new semi-implantable transcutaneous bone conduction device: clinical, surgical, and audiologic outcomes in patients with congenital ear canal atresia. Otol Neurotol. 2013; Jul. 34(5):927–34.8. Hol MK, Nelissen RC, Agterberg MJ, Cremers CW, Snik AF. Comparison between a new implantable transcutaneous bone conductor and percutaneous bone-conduction hearing implant. Otol Neurotol. 2013; Aug. 34(6):1071–5.
Article9. Deveze A, Rossetto S, Meller R, Sanjuan Puchol M. Switching from a percutaneous to a transcutaneous bone anchored hearing system: the utility of the fascia temporalis superficialis pedicled flap in case of skin intolerance. Eur Arch Otorhinolaryngol. 2015; Sep. 272(9):2563–9.
Article10. Dimitriadis PA, Farr MR, Allam A, Ray J. Three year experience with the cochlear BAHA attract implant: a systematic review of the literature. BMC Ear Nose Throat Disord. 2016; Oct. 16:12.
Article11. Gawecki W, Stieler OM, Balcerowiak A, Komar D, Gibasiewicz R, Karlik M, et al. Surgical, functional and audiological evaluation of new Baha(®) Attract system implantations. Eur Arch Otorhinolaryngol. 2016; Oct. 273(10):3123–30.
Article12. Morgan DE, Dirks DD, Bower DR. Suggested threshold sound pressure levels for frequency-modulated (warble) tones in the sound field. J Speech Hear Disord. 1979; Feb. 44(1):37–54.13. Kong TH, Park YA, Seo YJ. Image-guided implantation of the BonebridgeTM with a surgical navigation: a feasibility study. Int J Surg Case Rep. 2017; 30:112–7.14. Kim G, Ju HM, Lee SH, Kim HS, Kwon JA, Seo YJ. Efficacy of bone-anchored hearing aids in single-sided deafness: a systematic review. Otol Neurotol. 2017; Apr. 38(4):473–83.
Article15. Reddy-Kolanu G, Marshall A. Implantation of the Cochlear Baha(®) 4 Attract system through a linear incision. Ann R Coll Surg Engl. 2016; Jul. 98(6):437–8.
Article16. Brant JA, Gudis D, Ruckenstein MJ. Results of Baha® implantation using a small horizontal incision. Am J Otolaryngol. 2013; Nov-Dec. 34(6):641–5.
Article17. Guignard J, Arnold A, Weisstanner C, Caversaccio M, Stieger C. A bone-thickness map as a guide for bone-anchored port implantation surgery in the temporal bone. Materials (Basel). 2013; Nov. 6(11):5291–301.
Article18. Gonzales MB, Hufana VD. An anatomic study of the Asterion as a landmark for the location of the transverse-sigmoid sinus junction in Filipinos. Skull Base. 2008; 18(S 01):A227.
Article19. Ucerler H, Govsa F. Asterion as a surgical landmark for lateral cranial base approaches. J Craniomaxillofac Surg. 2006; Oct. 34(7):415–20.
Article20. Verstraeten N, Zarowski AJ, Somers T, Riff D, Offeciers EF. Comparison of the audiologic results obtained with the bone-anchored hearing aid attached to the headband, the testband, and to the “snap” abutment. Otol Neurotol. 2009; Jan. 30(1):70–5.
Article21. Briggs R, Van Hasselt A, Luntz M, Goycoolea M, Wigren S, Weber P, et al. Clinical performance of a new magnetic bone conduction hearing implant system: results from a prospective, multicenter, clinical investigation. Otol Neurotol. 2015; Jun. 36(5):834–41.22. Hwang JS, Kim KH, Lee JH. Factors affecting sentence-in-noise recognition for normal hearing listeners and listeners with hearing loss. J Audiol Otol. 2017; Jul. 21(2):81–7.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Novel Surgical Technique for BAHA® Attract Implantation
- Surgical and Audiologic Comparison Between Sophono and Bone-Anchored Hearing Aids Implantation
- Hearing Rehabilitation Using Bone Conduction Implants in Patients With Single-Sided Deafness After Vestibular Schwannoma Removal
- Single Vertical Incision Technique without Skin Thinning for the Bone Anchored Hearing Aid Surgery
- Change of Incision Wound after Folded Intraocular Lens Insertion Through 4.0 and 3.2 mmWidth Scleral Tunnel Incision
