Surgical and Audiologic Comparison Between Sophono and Bone-Anchored Hearing Aids Implantation
- Affiliations
-
- 1Soree Ear Clinic, Seoul, Korea. earclinic@hanmail.net
- 2Department of Otorhinolaryngology, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2166278
- DOI: http://doi.org/10.21053/ceo.2016.9.1.21
Abstract
OBJECTIVES
Bone-anchored hearing aids (BAHA) occasionally cause soft tissue problems due to abutment. Because Sophono does not have abutment penetrating skin, it is thought that Sophono has no soft tissue problem relating to abutment. On the other hand, transcutaneous device's output is reported to be 10 to 15 dB lower than percutaneous device. Therefore, in this study, Sophono and BAHA were compared to each other from surgical and audiological points of view.
METHODS
We retrospectively reviewed the medical records of 9 Sophono patients and 10 BAHA patients. In BAHA cases, single vertical incision without skin thinning technique was done. We compared Sophono to BAHA by operation time, wound healing time, postoperative complications, postoperative hearing gain after switch on, and postoperative air-bone gap.
RESULTS
The mean operation time was 60 minutes for Sophono and 25 minutes for BAHA. The wound healing time was 14 days for Sophono and 28 days for BAHA. No major intraoperative complication was observed. Skin problem was not observed in the 2 devices for the follow-up period. Postoperative hearing gain of bilateral aural atresia patients was 39.4 dB for BAHA (n=4) and 25.5 dB for Sophono (n=5). However, the difference was not statistically significant. In all patients included in this study, the difference of air-bone gap between two groups was 16.6 dB at 0.5 kHz and 18.2 dB at 4 kHz. BAHA was statistically significantly better than Sophono.
CONCLUSION
Considering the audiologic outcome, BAHA users were thought to have more audiologic benefit than Sophono users. However, Sophono had advantages over BAHA with abutment in cosmetic outcome. Sophono needed no daily skin maintenance and soft tissue complication due to abutment would not happen in Sophono. Therefore, a full explanation about each device is necessary before deciding implantation.
Keyword
MeSH Terms
Figure
-
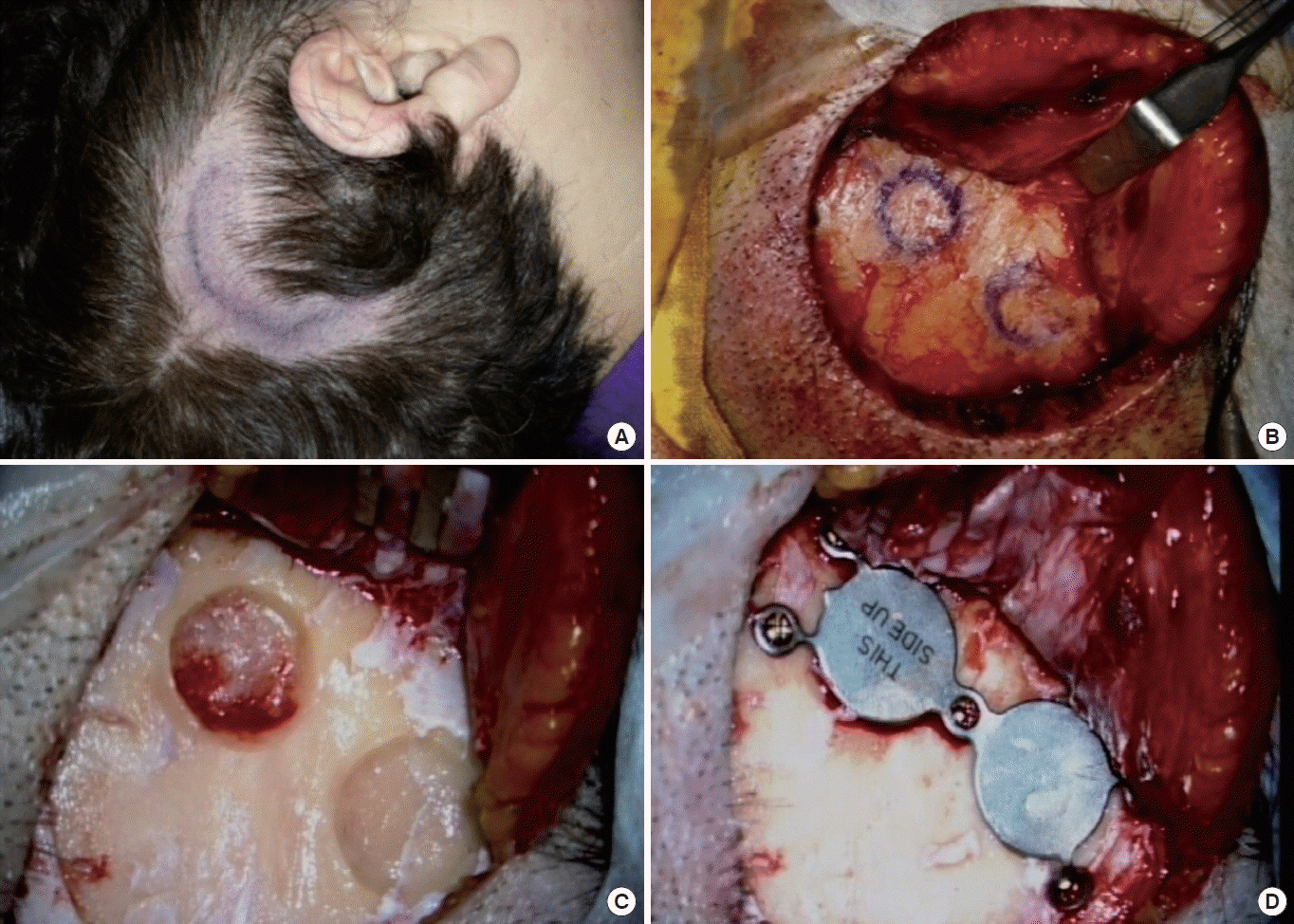
Fig. 1. Operative procedure of Sophono. (A) The curved skin incision is marked using the template. Seven to 8 cm-sized curved incision was made along the template at the postauricular area. (B) The pericranium was dissected and elevated anteriorly enough to drill and insert the implantable component. (C) Well for implantable component was drilled. The recommended size of the well was 2.5 mm in depth and 10 mm in diameter. It could be gazed by the template. (D) Another drillings for five screws were done. After then, the implant was fixed by five titanium screws.
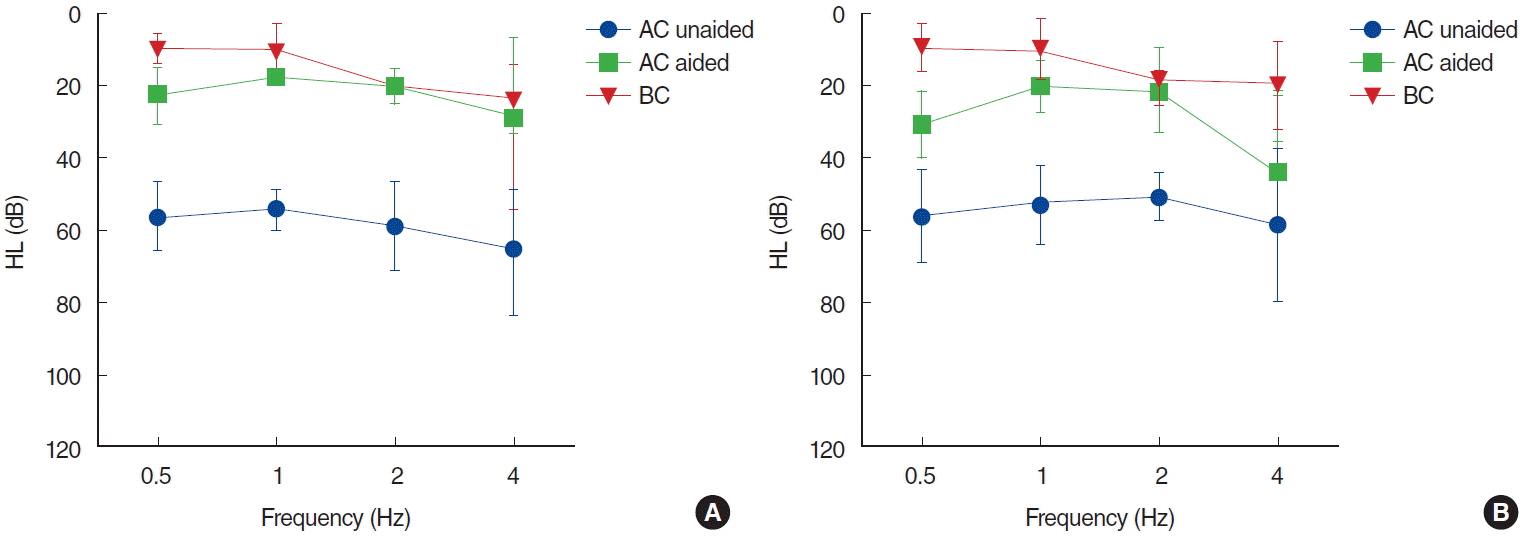
Fig. 2. The comparison of the bilateral aural atresia patients (Sophono, n=5; BAHA, n=4). (A) Unaided mean AC hearing of BAHA was 62.8 dB and aided mean free-field AC hearing was 22.2 dB. Postoperative hearing gain was 40.6 dB. (B) Unaided mean AC hearing of Sophono was 53.7 dB and aided mean free-field AC hearing was 23.7 dB. Postoperative hearing gain was 30 dB. BAHA was better than the Sophono in the postoperative hearing gain, but the difference was not statistically significant. BAHA, bone-anchored hearing aids; AC, air-conduction; BC, bone-conduction; HL, hearing loss.
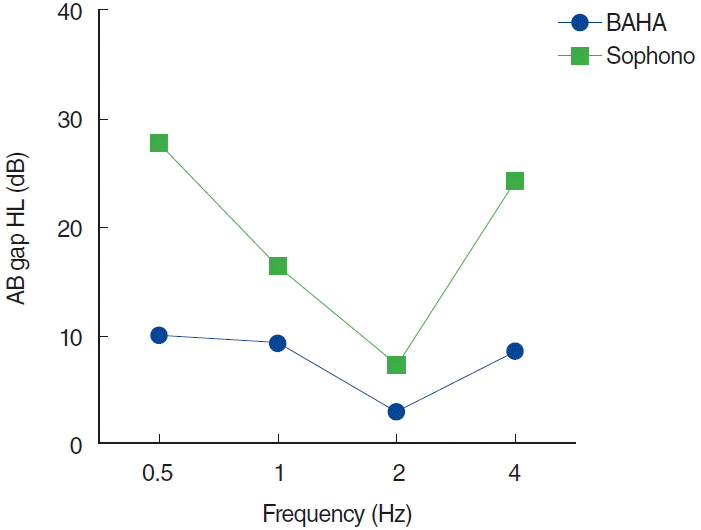
Fig. 3. The postoperative AB gap comparison of all patients included in this study (Sophono, n=9; BAHA, n=10). We compared postoperative AB gap of Sophono and BAHA according to the frequency. BAHA was better than Sophono in the AB gap, and the difference of 0.5 and 4 kHz was statistically significant. AB, air-bone; BAHA, bone-anchored hearing aids; HL, hearing loss.
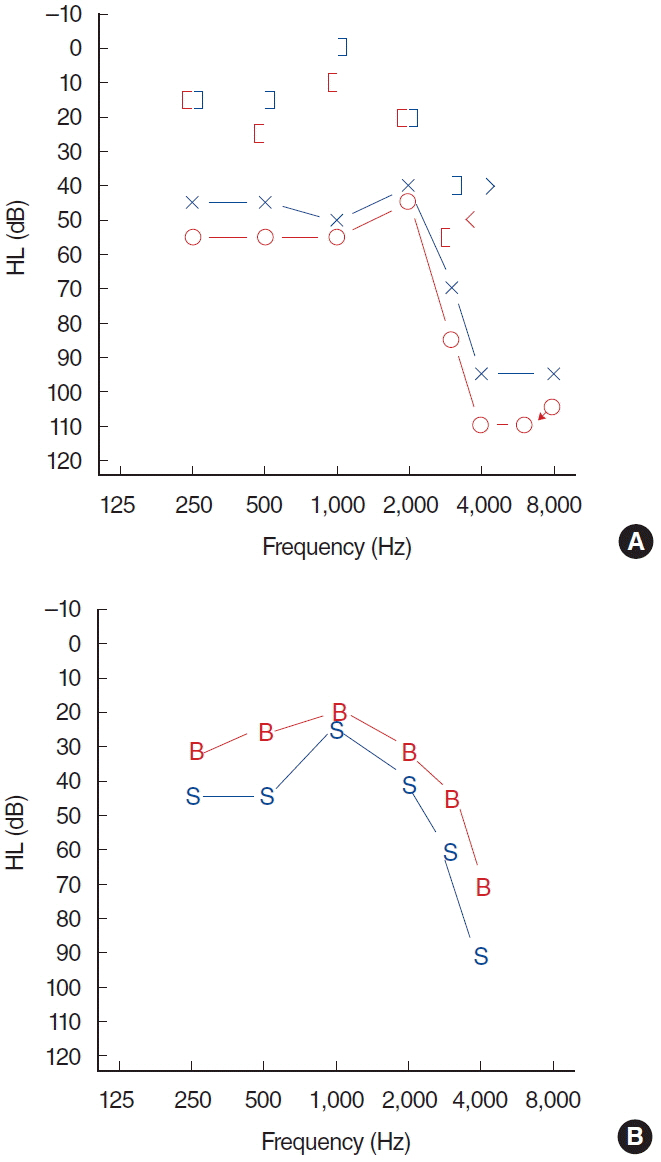
Fig. 4. The audiogram of patient who was implanted both Sophono and BAHA. Hearing gain of BAHA was better than Sophono in all audiologic frequencies. (A) Preoperative audiogram. (B) Aided audiogram. BAHA, bone-anchored hearing aids; B, BAHA; S, Sophono; HL, hearing loss.
Cited by 2 articles
-
Current Developments and Challenge of Implantable Bone Conduction Hearing Aids
Saea Kim, Woojae Han
Korean J Otorhinolaryngol-Head Neck Surg. 2018;61(2):67-75. doi: 10.3342/kjorl-hns.2017.00864.Comparison of Aided and Unaided Thresholds and Selection Processes of Contralateral Routing of Signal Hearing Aids and Implantable Bone Conduction Devices in Patients with Asymmetric Hearing Loss
Yong Han Kim, Ho-Jun Lee, Mi Rye Bae, Ja Yoon Ku, Chol Ho Shin, Hong Ju Park
Korean J Otorhinolaryngol-Head Neck Surg. 2019;62(3):157-164. doi: 10.3342/kjorl-hns.2018.00248.
Reference
-
1. House JW, Kutz JW Jr. Bone-anchored hearing aids: incidence and management of postoperative complications. Otol Neurotol. 2007; Feb. 28(2):213–7.2. Wazen JJ, Young DL, Farrugia MC, Chandrasekhar SS, Ghossaini SN, Borik J, et al. Successes and complications of the Baha system. Otol Neurotol. 2008; Dec. 29(8):1115–9.
Article3. Hol MK, Nelissen RC, Agterberg MJ, Cremers CW, Snik AF. Comparison between a new implantable transcutaneous bone conductor and percutaneous bone-conduction hearing implant. Otol Neurotol. 2013; Aug. 34(6):1071–5.
Article4. Zwartenkot JW, Snik AF, Mylanus EA, Mulder JJ. Amplification options for patients with mixed hearing loss. Otol Neurotol. 2014; Feb. 35(2):221–6.
Article5. Shin JW, Park HJ, Lee SC, Park HQ, Lee HK. Single vertical incision technique without skin thinning for the bone anchored hearing aid surgery. Korean J Otorhinolaryngol-Head Neck Surg. 2012; Mar. 55(3):151–4.
Article6. Hultcrantz M. Outcome of the bone-anchored hearing aid procedure without skin thinning: a prospective clinical trial. Otol Neurotol. 2011; Sep. 32(7):1134–9.7. Soo GM, Tong CF, Tsang SS, Van Hasselt CA. The Hong Kong incision (direct percutaneous Baha surgery without soft tissue reduction or skin grafting): early results. In : The 2nd International Symposium on Bone Conduction Hearing - Craniofacial osseo-integration; 2009 Jun 11th–13th; Gothenburg, Sweden. 2009. 33–4.8. Siegert R. Partially implantable bone conduction hearing aids without a percutaneous abutment (Otomag): technique and preliminary clinical results. Adv Otorhinolaryngol. 2011; 71:41–6.
Article9. O’Niel MB, Runge CL, Friedland DR, Kerschner JE. Patient outcomes in magnet-based implantable auditory assist devices. JAMA Otolaryngol Head Neck Surg. 2014; Jun. 140(6):513–20.
Article10. Magliulo G, Turchetta R, Iannella G, Valperga di Masino R, de Vincentiis M. Sophono Alpha System and subtotal petrosectomy with external auditory canal blind sac closure. Eur Arch Otorhinolaryngol. 2015; Sep. 272(9):2183–90.
Article11. Denoyelle F, Leboulanger N, Coudert C, Mazzaschi O, Loundon N, Vicaut E, et al. New closed skin bone-anchored implant: preliminary results in 6 children with ear atresia. Otol Neurotol. 2013; Feb. 34(2):275–81.12. Siegert R, Kanderske J. A new semi-implantable transcutaneous bone conduction device: clinical, surgical, and audiologic outcomes in patients with congenital ear canal atresia. Otol Neurotol. 2013; Jul. 34(5):927–34.13. Verstraeten N, Zarowski AJ, Somers T, Riff D, Offeciers EF. Comparison of the audiologic results obtained with the bone-anchored hearing aid attached to the headband, the testband, and to the “snap” abutment. Otol Neurotol. 2009; Jan. 30(1):70–5.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hearing Rehabilitation with Sophono(R) in Patients with Unilateral Hearing Loss after Meningioma Removal
- Current Developments and Challenge of Implantable Bone Conduction Hearing Aids
- Experience of BAHA(Bone Anchored Hearing Aid) Surgery
- Hearing Rehabilitation Experiences With Osia®2 Bone Conduction Hearing Implant in Patients With Iatrogenic Unilateral Hearing Loss
- Subjective and Audiologic Results of Bone Anchored Hearing Aids (BAHA)
