Steroid-resistant sarcoid myositis thatwas successfully treated with oralmethotrexate
- Affiliations
-
- 1Department of Neurology, Research Institute for Convergence of Biomedical Research, Pusan National University Yangsan Hospital, Yangsan, Korea
- 2Department of Neurology, Good Gang-An Hospital, Busan, Korea
- 3Department of Neurology, Kosin University College of Medicine, Busan, Korea
- 4Department of Neurology, Pusan National University Hospital, Busan, Korea
- 5Department of Neurology, Pusan National University School of Medicine, Yangsan, Korea
- KMID: 2500304
- DOI: http://doi.org/10.14253/acn.2020.22.1.41
Abstract
- Acute sarcoid myositis is rarely complicated by sarcoidosis, and steroid therapy is considered the standard treatment. We experienced a patient with acute sarcoid myositis who did not respond to aggressive high-dose corticosteroid therapy, but showed a dramatic improvement after the addition of weekly low-dose oral methotrexate (MTX). This intervention allowed the resumption of normal daily activities after 6 months. Our case strongly suggests that MTX should be considered in patients with acute sarcoid myositis that is resistant to corticosteroid therapy.
Keyword
Figure
-
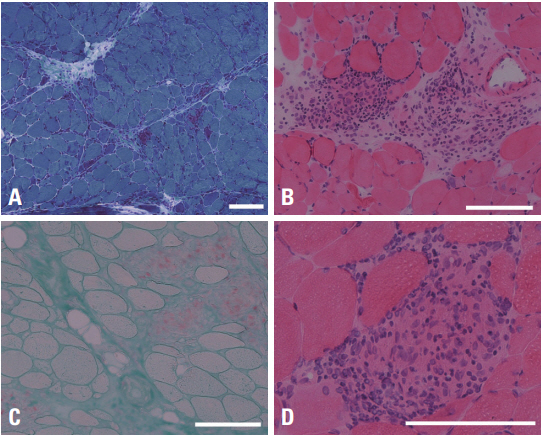
Fig. 1. Muscle biopsy findings of the patient. Noncaseating granulomas with multinucleated giant cells and infiltrating lymphocytes are observed. In addition, many muscle fibers, especially in the periphery of the muscle fascicles, are atrophic and there are scattered necrotic and regenerating fibers. (A) Modified Gomori-trichrome stain (×40), (B) hematoxylin-eosin stain (×100), (C) acid phosphatase stain (×100), (D) hematoxylin-eosin stain (×200). A white bar indicates 100 μm.
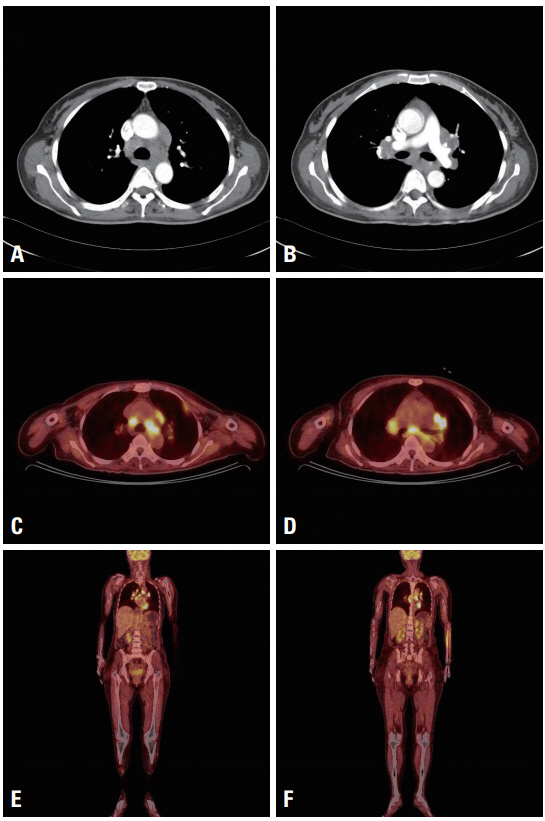
Fig. 2. A chest computed tomography image shows parenchymal opacifications in the lung and bilateral hilar enlargement with enlarged multiple mediastinal lymph nodes (A, B). Whole-body flourodeoxyglucose positron emission tomography (FDG-PET) shows abnormal FDG uptake in mediastinal lymph nodes and left pleura. In extremities, no abnormal FDG uptake is observed in other tissue including skeletal muscle. An increased FDG uptake in left forearm area is considered as an artifact at injection site (C-F).
Reference
-
1. Silverstein A, Siltzbach LE. Muscle involvement in sarcoidosis. Asymptomatic, myositis, and myopathy. Arch Neurol. 1969; 21:235–241.2. Fujita H, Ishimatsu Y, Motomura M, Kakugawa T, Sakamoto N, Hayashi T, et al. A case of acute sarcoid myositis treated with weekly low-dose methotrexate. Muscle Nerve. 2011; 44:994–999.
Article3. Loe MJ, Subramaniam RM, Kalra S, Tiegs RD, Mullan BP, Utz JP. F-18 fluorodeoxyglucose positron emission tomography/computed tomography in the diagnosis of chronic myopathic sarcoidosis. Clin Nucl Med. 2010; 35:22–23.4. Marie I, Lahaxe L, Vera P, Edet-Samson A. Follow-up of muscular sarcoidosis using fluorodeoxyglucose positron emission tomography. QJM. 2010; 103:1000–1002.
Article5. Akaike G, Itani M, Shah H, Ahuja J, Yilmaz Gunes B, Assaker R, et al. PET/CT in the diagnosis and workup of sarcoidosis: focus on atypical manifestations. Radiographics. 2018; 38:1536–1549.6. Baughman RP, Lower EE. A clinical approach to the use of methotrexate for sarcoidosis. Thorax. 1999; 54:742–746.
Article
