A Case of Solitary Fibrous Tumor of Subungual Region
- Affiliations
-
- 1Department of Dermatology, Hallym University Sacred Heart Hospital, Anyang, Korea. dermakkh@naver.com
- KMID: 2471341
- DOI: http://doi.org/10.5021/ad.2020.32.2.146
Abstract
- Solitary fibrous tumor (SFT) is a relatively uncommon mesenchymal neoplasm that usually arises in the pleura, but also has been reported in numerous extrapleural locations, including cutaneous site. The skin lesion presents as a circumscribed nodule or tumor, mainly on the head and neck. A 41-year-old male presented with 6 months history of nail lesion without symptom on the left third finger. The lesion is slightly yellowish discoloration with subungual erythematous nodule and distal onycholysis. Biopsy specimen from the nail lesion showed the spindle cells form patternless pattern with hypercellular and hypocellular area. And small blood vessels and dilated vascular spaces were present. The result of special stain for specimen showed that positive for CD34, Bcl-2, and CD99 but negative for S-100, FactorXIIIa, and smooth muscle action. Recognition of this uncommon location of SFT is important because of possible confusion with other subungual tumors, including glomus tumor, fibroma and other fibrohistiocytic tumors like dermatofibrosarcoma protuberans, superficial acral fibromyxoma and cellular digital fibroma. Here in, we report a case of SFT of subungual region. We think this case is interesting because of uncommon location and may be helpful to more understand the character of this disease.
Keyword
MeSH Terms
Figure
-
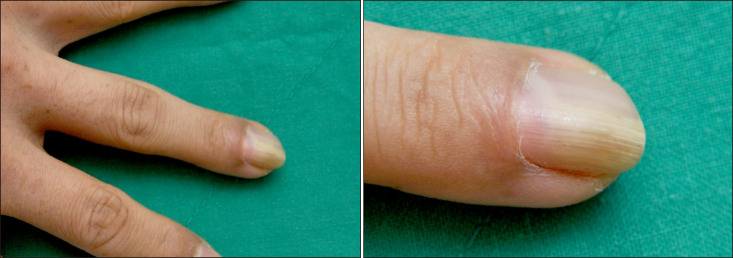
Fig. 1 Slightly yellowish discoloration with hypertrophic nail and distal onycholysis and erythematous subungual nodule on the proximal nail fold of left third finger.
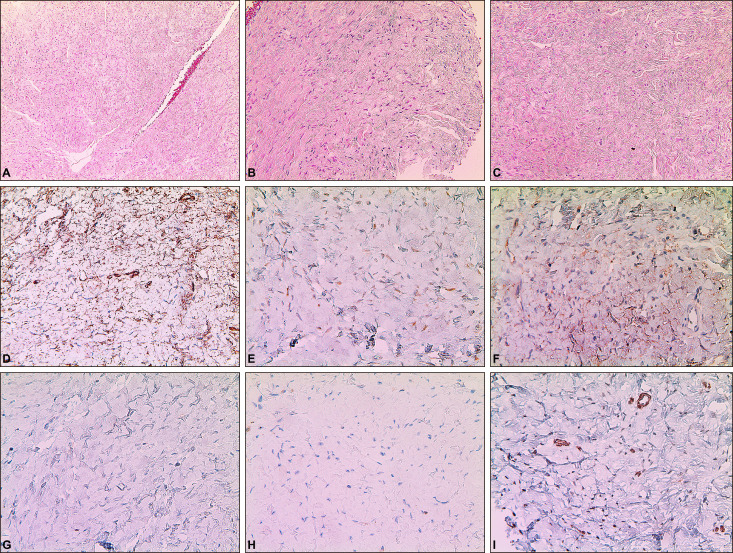
Fig. 2 (A) The biopsy specimen shows proliferation of spindle cells and several small blood vessels and dilated vascular spaces are present (H&E, ×100). (B) The spindle cells form patternless pattern with hypercellular areas (H&E, ×200). (C) The spindle cells form patternless pattern with hypocellular areas (H&E, ×200). (D) The tumor cells are diffusely positive for CD34 (×400). (E) The tumor cells are positive for Bcl-2 (×400). (F) The tumor cells are diffusely positive for CD99 (×400). (G) The tumor cells are negative for S-100 (×400). (H) The tumor cells are negative for FactorXIIIa (×400). (I) The tumor cells are negative for SMA (×400).
Reference
-
1. Soldano AC, Meehan SA. Cutaneous solitary fibrous tumor: a report of 2 cases and review of the literature. Am J Dermatopathol. 2008; 30:54–58. PMID: 18212546.
Article2. Erdag G, Qureshi HS, Patterson JW, Wick MR. Solitary fibrous tumors of the skin: a clinicopathologic study of 10 cases and review of the literature. J Cutan Pathol. 2007; 34:844–850. PMID: 17944724.
Article3. Okamura JM, Barr RJ, Battifora H. Solitary fibrous tumor of the skin. Am J Dermatopathol. 1997; 19:515–518. PMID: 9335244.
Article4. Oh YJ, Lew BL, Sim WY. Primary cutaneous solitary fibrous tumor. Korean J Dermatol. 2011; 49:1093–1097.5. Chang SE, Bae GY, Choi JH, Sung KJ, Moon KC, Koh JK, et al. Cutaneous solitary fibrous tumour with myxoid stroma. Br J Dermatol. 2002; 147:1267–1269. PMID: 12452886.
Article6. Lee HJ, Lee SH, Roh MR. Cutaneous myxoid solitary fibrous tumour. Clin Exp Dermatol. 2012; 37:197–199. PMID: 22092338.
Article7. Suster S, Nascimento AG, Miettinen M, Sickel JZ, Moran CA. Solitary fibrous tumors of soft tissue. A clinicopathologic and immunohistochemical study of 12 cases. Am J Surg Pathol. 1995; 19:1257–1266. PMID: 7573687.8. Morgan MB, Smoller BR. Solitary fibrous tumors are immunophenotypically distinct from mesothelioma(s). J Cutan Pathol. 2000; 27:451–454. PMID: 11028815.
Article9. Yoshida Y, Kubota Y, Yamaguchi T, Iwasaki H, Nakayama J. Subcutaneous solitary fibrous tumor. J Dermatol. 2004; 31:1018–1022. PMID: 15801268.
Article10. Terada T. Solitary fibrous tumor of the shoulder showing diverse distinct histologic patterns. Int J Dermatol. 2011; 50:208–211. PMID: 21244389.
Article11. Hata H, Natsuga K, Aoyagi S, Homma E, Shimizu H. Solitary fibrous tumour fluctuating in size with menstrual cycle. Clin Exp Dermatol. 2014; 39:753–755. PMID: 24986672.
Article12. Lee JY, Park SE, Shin SJ, Kim CW, Kim SS, Kim KH. Solitary fibrous tumor with myxoid stromal change. Am J Dermatopathol. 2015; 37:570–573. PMID: 25140663.
Article13. Lee JY, Kim DH, Seo KJ, Jung SN. A solitary fibrous tumor (cellular form) of the ankle. J Foot Ankle Surg. 2016; 55:829–831. PMID: 25979291.
Article14. Sidney LE, Branch MJ, Dunphy SE, Dua HS, Hopkinson A. Concise review: evidence for CD34 as a common marker for diverse progenitors. Stem Cells. 2014; 32:1380–1389. PMID: 24497003.
Article15. Sawaya JL, Khachemoune A. Superficial acral fibromyxoma. Int J Dermatol. 2015; 54:499–508. PMID: 25772615.
Article16. Lee JY, Park SE, Shin SJ, Kim CW, Kim SS. Diagnostic pitfalls of differentiating cellular digital fibroma from superficial acral fibromyxoma. Ann Dermatol. 2015; 27:462–464. PMID: 26273171.
Article17. Doyle LA, Vivero M, Fletcher CD, Mertens F, Hornick JL. Nuclear expression of STAT6 distinguishes solitary fibrous tumor from histologic mimics. Mod Pathol. 2014; 27:390–395. PMID: 24030747.
Article18. Anders JO, Aurich M, Lang T, Wagner A. Solitary fibrous tumor in the thigh: review of the literature. J Cancer Res Clin Oncol. 2006; 132:69–75. PMID: 16283380.
Article19. Nielsen GP, O'Connell JX, Dickersin GR, Rosenberg AE. Solitary fibrous tumor of soft tissue: a report of 15 cases, including 5 malignant examples with light microscopic, immunohistochemical, and ultrastructural data. Mod Pathol. 1997; 10:1028–1037. PMID: 9346183.
