Closure of oroantral fistula: a review of local flap techniques
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, School of Dentistry, Kyung Hee University, Seoul, Korea. kwony@khu.ac.kr
- KMID: 2471113
- DOI: http://doi.org/10.5125/jkaoms.2020.46.1.58
Abstract
- Oroantral fistula (OAF), also termed oroantral communication, is an abnormal condition in which there is a communicating tract between the maxillary sinus and the oral cavity. The most common causes of this pathological communication are known to be dental implant surgery and extraction of posterior maxillary teeth. The purpose of this article is to describe OAF; introduce the approach algorithm for the treatment of OAF; and review the fundamental surgical techniques for fistula closure with their advantages and disadvantages. The author included a thorough review of the previous studies acquired from the PubMed database. Based on this review, this article presents cases of OAF patients treated with buccal flap, buccal fat pad (BFP), and palatal rotational flap techniques.
MeSH Terms
Figure
-
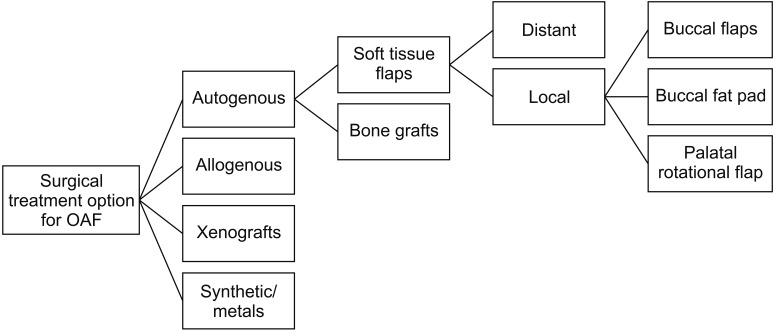
Fig. 1 Treatment modalities for oroantral fistula (OAF) closure. Modified from the article of Parvini et al.3 (Int J Implant Dent 2018;4:40) in accordance with the Creative Commons Attribution 4.0 International (CC BY 4.0) license.
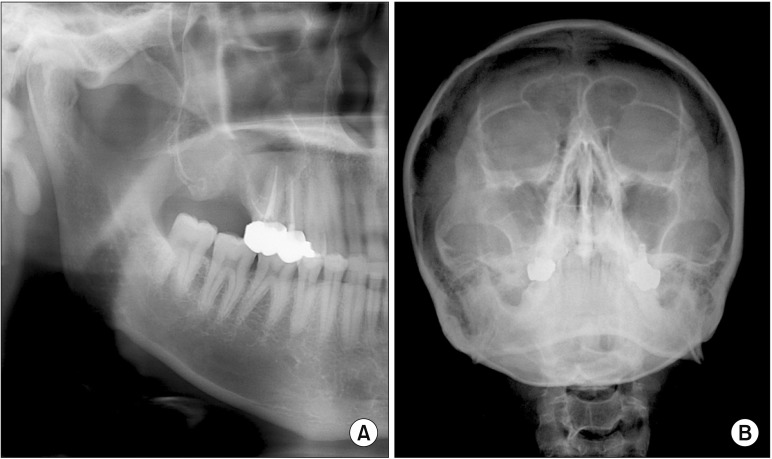
Fig. 2 A. Panorama shows a suspicious lesion at the extraction site of the posterior maxilla. B. Opacity of the right maxillary sinus is decreased on Waters' view due to the sinus infection.
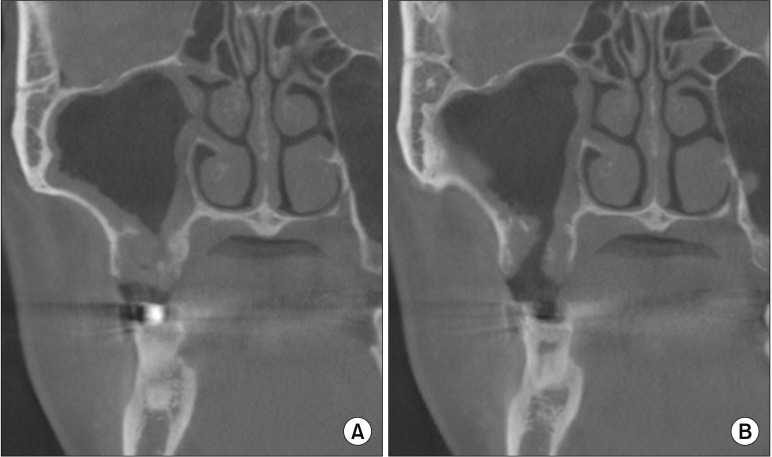
Fig. 3 Cone-beam computed tomography imaging confirms the connected tract (A) and the sinus infection (B) on the right maxillary sinus.
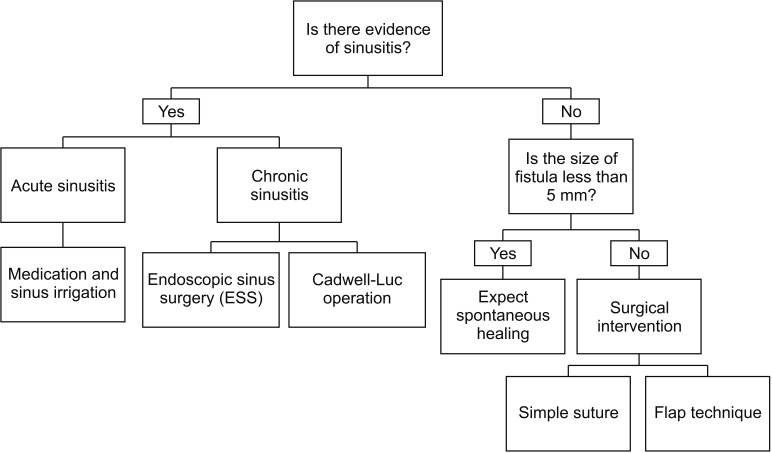
Fig. 4 Approach algorithm for the treatment of oroantral fistula.
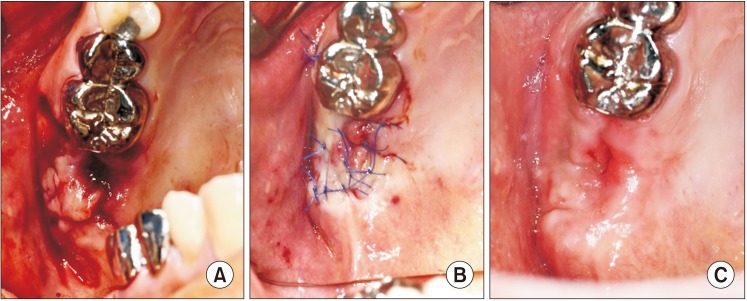
Fig. 5 A. shows a fistula the size of a single tooth on the second premolar region of the maxilla. B. The buccal sliding flap covering over the fistula and sutured with the palatal mucosa can be seen. C. Complete healing was obtained at three weeks after the surgery.
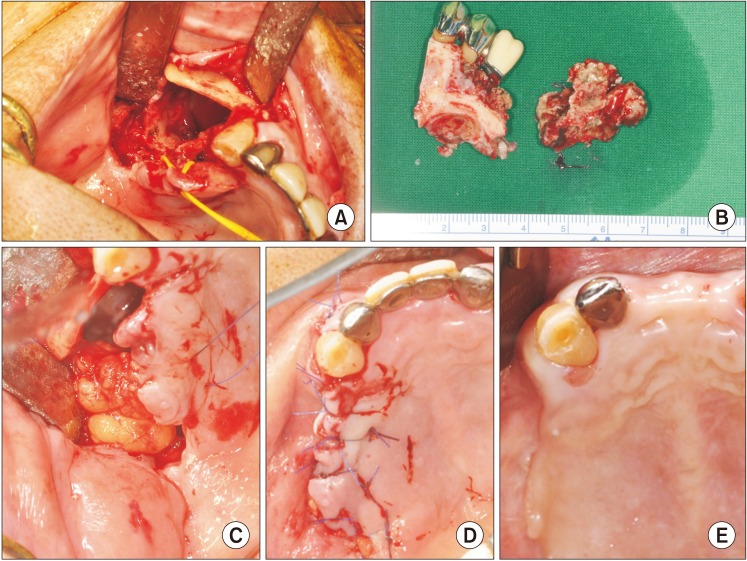
Fig. 6 A, B. Partial maxillectomy was performed to remove the necrotic region of the maxilla. C. Harvest of the abundant amount of the buccal fat pad (BFP). D. The defect was covered with the BFP and oral mucosa by double-layered suture. E. Complete healing was observed, and no signs of complications were noted at 11 weeks after the surgery.
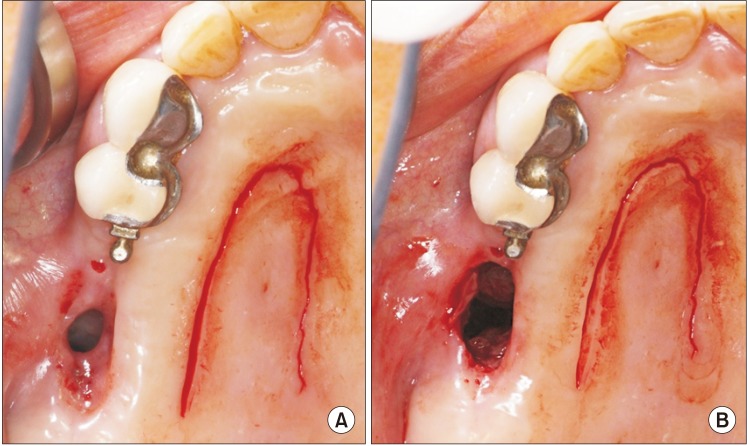
Fig. 7 A, B. Circular excision of the fistula tract reveals a larger entrance than as suggested from the outside.
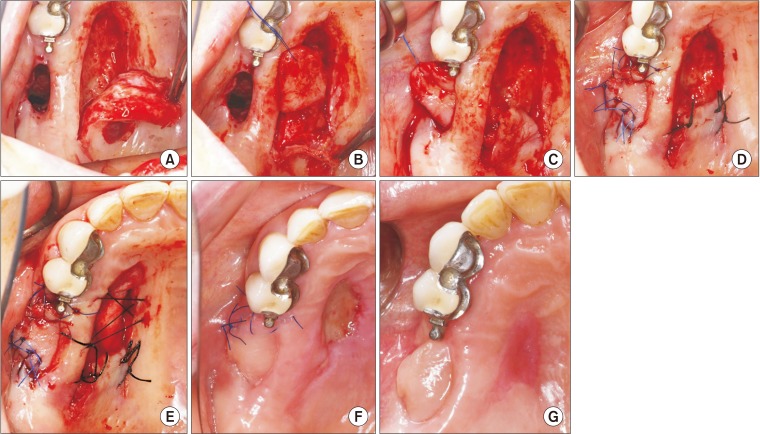
Fig. 8 A. Full-thickness palatal harvest includes the greater palatine artery. B. Subepithelial dissection of the rotating region of the flap. C. The flap was rotated and placed through the fistula tract underneath the tunnel. D. The flap was sutured to the remaining buccal mucosa and, also, the rotated area of the flap was sutured to limit undesired movement of the flap during the healing period. E. The collagen sponge was used to cover the denuded donor site. F. The secondary wound healing of the donor site can be seen. G. Complete healing without complications was observed at two months of follow-up.
Reference
-
1. Yalççn S, Oncü B, Emes Y, Atalay B, Aktaş I. Surgical treatment of oroantral fistulas: a clinical study of 23 cases. J Oral Maxillofac Surg. 2011; 69:333–339. PMID: 21145640.2. Visscher SH, van Minnen B, Bos RR. Closure of oroantral communications: a review of the literature. J Oral Maxillofac Surg. 2010; 68:1384–1391. PMID: 20227153.
Article3. Parvini P, Obreja K, Sader R, Becker J, Schwarz F, Salti L. Surgical options in oroantral fistula management: a narrative review. Int J Implant Dent. 2018; 4:40. PMID: 30588578.
Article4. Dym H, Wolf JC. Oroantral communication. Oral Maxillofac Surg Clin North Am. 2012; 24:239–247. viii–ix. PMID: 22503070.
Article5. Hernando J, Gallego L, Junquera L, Villarreal P. Oroantral communications. A retrospective analysis. Med Oral Patol Oral Cir Bucal. 2010; 15:e499–e503. PMID: 20038901.
Article6. Rehrmann A. [Eine methode zur schliessung von kieferhöhlenperforationen]. Dtsch Zahnärztl Wschr. 1936; 39:1136–1138. German.7. Killey HC, Kay LW. Observations based on the surgical closure of 362 oro-antral fistulas. Int Surg. 1972; 57:545–549. PMID: 5042434.8. von Wowern N. Closure of oroantral fistula with buccal flap: Rehrmann versus Môczár. Int J Oral Surg. 1982; 11:156–165. PMID: 6813275.
Article9. Haanaes HR, Pedersen KN. Treatment of oroantral communication. Int J Oral Surg. 1974; 3:124–132. PMID: 4209425.
Article10. Martín-Granizo R, Naval L, Costas A, Goizueta C, Rodriguez F, Monje F, et al. Use of buccal fat pad to repair intraoral defects: review of 30 cases. Br J Oral Maxillofac Surg. 1997; 35:81–84. PMID: 9146863.
Article11. el-Hakim IE, el-Fakharany AM. The use of the pedicled buccal fat pad (BFP) and palatal rotating flaps in closure of oroantral communication and palatal defects. J Laryngol Otol. 1999; 113:834–838. PMID: 10664688.
Article12. Rapidis AD, Alexandridis CA, Eleftheriadis E, Angelopoulos AP. The use of the buccal fat pad for reconstruction of oral defects: review of the literature and report of 15 cases. J Oral Maxillofac Surg. 2000; 58:158–163. PMID: 10670594.
Article13. Egyedi P. Utilization of the buccal fat pad for closure of oro-antral and/or oro-nasal communications. J Maxillofac Surg. 1977; 5:241–244. PMID: 338848.
Article14. Arce K. Buccal fat pad in maxillary reconstruction. Atlas Oral Maxillofac Surg Clin North Am. 2007; 15:23–32. PMID: 17434059.
Article15. Stajcić Z. The buccal fat pad in the closure of oro-antral communications: a study of 56 cases. J Craniomaxillofac Surg. 1992; 20:193–197. PMID: 1401089.16. Baumann A, Ewers R. Application of the buccal fat pad in oral reconstruction. J Oral Maxillofac Surg. 2000; 58:389–392. discussion 392–3. PMID: 10759118.
Article17. Yang S, Jee YJ, Ryu DM. Reconstruction of large oroantral defects using a pedicled buccal fat pad. Maxillofac Plast Reconstr Surg. 2018; 40:7. PMID: 29637060.
Article18. Parvini P, Obreja K, Begic A, Schwarz F, Becker J, Sader R, et al. Decision-making in closure of oroantral communication and fistula. Int J Implant Dent. 2019; 5:13. PMID: 30931487.
Article19. Paterson C, Thomson MC, Caldwell B, Young R, McLean A, Porteous S, et al. Radiotherapy-induced xerostomia: a randomised, double-blind, controlled trial of Visco-ease™ oral spray compared with placebo in patients with cancer of the head and neck. Br J Oral Maxillofac Surg. 2019; 57:1119–1125. PMID: 31672256.
Article20. Dirix P, Nuyts S, Van den Bogaert W. Radiation-induced xerostomia in patients with head and neck cancer: a literature review. Cancer. 2006; 107:2525–2534. PMID: 17078052.21. Dirix P, Nuyts S, Vander Poorten V, Delaere P, Van den Bogaert W. The influence of xerostomia after radiotherapy on quality of life: results of a questionnaire in head and neck cancer. Support Care Cancer. 2008; 16:171–179. PMID: 17618467.22. Vissink A, Mitchell JB, Baum BJ, Limesand KH, Jensen SB, Fox PC, et al. Clinical management of salivary gland hypofunction and xerostomia in head-and-neck cancer patients: successes and barriers. Int J Radiat Oncol Biol Phys. 2010; 78:983–991. PMID: 20970030.
Article23. Tideman H, Bosanquet A, Scott J. Use of the buccal fat pad as a pedicled graft. J Oral Maxillofac Surg. 1986; 44:435–440. PMID: 3457926.
Article24. Wells DL, Capes JO. Complications of dentoalveolar surgery. In : Fonseca RJ, editor. Oral and maxillofacial surgery. Philadelphia: WB Saunders;2000. p. 432.25. Ehrl PA. Oroantral communication. Epicritical study of 175 patients, with special concern to secondary operative closure. Int J Oral Surg. 1980; 9:351–358. PMID: 6783559.26. Anavi Y, Gal G, Silfen R, Calderon S. Palatal rotation-advancement flap for delayed repair of oroantral fistula: a retrospective evaluation of 63 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003; 96:527–534. PMID: 14600685.
Article27. Jamali JA. Palatal flap. Oral Maxillofac Surg Clin North Am. 2014; 26:305–311. PMID: 25086692.
Article28. Ward BB. The palatal flap. Oral Maxillofac Surg Clin North Am. 2003; 15:467–473. vPMID: 18088697.
Article29. Hong SO, Shim GJ, Kwon YD. Novel approach to the maxillary sinusitis after sinus graft. Maxillofac Plast Reconstr Surg. 2017; 39:18. PMID: 28695114.
Article30. Er N, Tuncer HY, Karaca C, Copuroğlu S. Treatment of oroantral fistulas using bony press-fit technique. J Oral Maxillofac Surg. 2013; 71:659–666. PMID: 23507319.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Review of the healing mechanism of maxillary antrum after Caldwell-Luc operation and the case report of recurrent oroantral fistulaafter Caldwell-Luc operation with oroantral fistula closure
- A Case of Large Oroantral Fistula Repair Using Iliac Bone Plug
- A Case of Oroantral Fistula Complicating Fungal Sinusitis
- The double-barrier technique using platelet-rich fibrin for closure of oroantral fistulas
- Versatility of the pedicled buccal fat pad flap for the management of oroantral fistula: a retrospective study of 25 cases
