Bow Hunter's Syndrome Caused by Bilateral Dynamic Occlusion of the Subaxial Vertebral Arteries during Neck Extension
- Affiliations
-
- 1Department of Orthopaedic Surgery, Dankook University College of Medicine, Cheonan, Korea.
- 2Department of Orthopaedic Surgery, National Medical Center, Seoul, Korea. hosunghan.md@gmail.com
- KMID: 2470773
- DOI: http://doi.org/10.4055/jkoa.2020.55.1.85
Abstract
- Bow hunter's syndrome is a rare disease that shows the symptoms of vertebrobasilar insufficiency resulting from a dynamic obstruction or stenosis of the vertebral arteries during neck movement. This paper reports a case of a 59-year-old male who visited the emergency room with diplopia, tinnitus, and gait disturbance. Magnetic resonance imaging and angiography revealed a multiple cerebellar infarct, total obstruction of the right vertebral artery, and dynamic obstruction of the left vertebral artery during neck extension. As the infarction worsened, a thrombectomy was done. Posterior decompression and fusion at C5-6 were performed for the left vertebral artery. The left vertebral arterial patency was confirmed by intraoperative and postoperative angiography. No recurrence of the symptoms was observed for six months after surgery. Physicians need to pay attention to the diagnosis of vertebrobasilar insufficiency caused by an obstruction of the vertebral arteries during neck extension in cervical instability patients.
Keyword
MeSH Terms
Figure
-
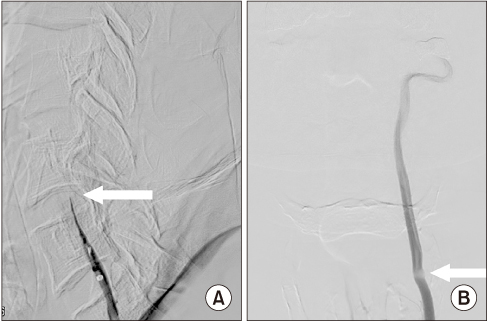
Figure 1 Initial transfemoral cerebral angiography images show occlusion of the vertebral arteries. (A) The right vertebral artery is completely occluded at the C5-6 disc level (arrow). (B) The left vertebral artery is partially occluded by the C6 superior articular process (arrow).
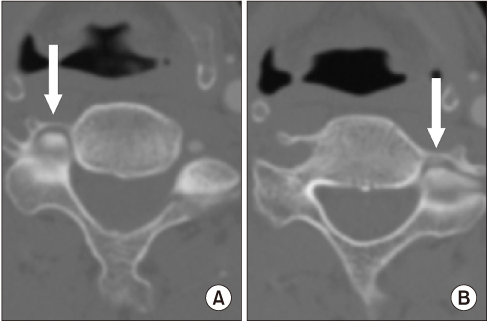
Figure 2 Preoperative computed tomography angiography shows a blockade of circulation at the transverse foramina. (A) The right superior articular process completely occludes the right vertebral artery (arrow). (B) The left superior articular process occludes approximately 80% of the left C5 transverse foramen (arrow).

Figure 3 Intraoperative microscopy images show that the defect produced by left total facetectomy at C5 (white asterisk)-6 (black asterisk) was repaired by an interpositional bone graft using an auto iliac bone block (arrow).
Figure 4 Intraoperative transfemoral cerebral angiography images show undisrupted blood flow of the left vertebral artery.
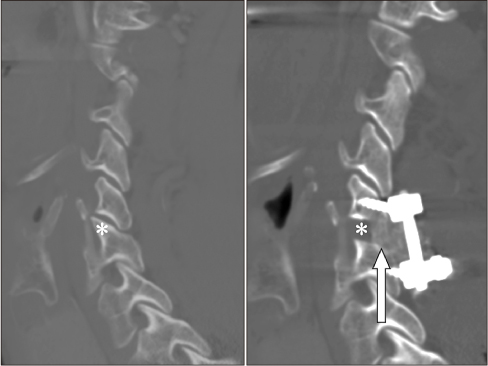
Figure 5 Postoperative computed tomography angiography shows complete resection of the left C6 superior articular process (asterisk) and successful decompression of the left vertebral artery. Interpositional bone block appears beautiful (arrow).
Reference
-
1. Sorensen BF. Bow hunter's stroke. Neurosurgery. 1978; 2:259–261.
Article2. Rastogi V, Rawls A, Moore O, et al. Rare etiology of Bow Hunter's syndrome and systematic review of literature. J Vasc Interv Neurol. 2015; 8:7–16.3. Yamamoto N, Kosaka H, Higashino K, et al. Vertebral lateral notch as optimal entry point for lateral mass screwing using modified Roy-Camille technique. Asian Spine J. 2018; 12:272–276.
Article4. Suh BG, Padua MR, Riew KD, et al. A new technique for reduction of atlantoaxial subluxation using a simple tool during posterior segmental screw fixation: clinical article. J Neurosurg Spine. 2013; 19:160–166.5. Zaidi HA, Albuquerque FC, Chowdhry SA, Zabramski JM, Ducruet AF, Spetzler RF. Diagnosis and management of bow hunter's syndrome: 15-year experience at barrow neurological institute. World Neurosurg. 2014; 82:733–738.6. Cornelius JF, George B, N'dri Oka D, Spiriev T, Steiger HJ, Hänggi D. Bow-hunter's syndrome caused by dynamic vertebral artery stenosis at the cranio-cervical junction–a management algorithm based on a systematic review and a clinical series. Neurosurg Rev. 2012; 35:127–135. discussion 135.
Article7. Duan G, Xu J, Shi J, Cao Y. Advances in the pathogenesis, diagnosis and treatment of Bow Hunter's syndrome: a comprehensive review of the literature. Interv Neurol. 2016; 5:29–38.
Article8. Darkhabani MZ, Thompson MC, Lazzaro MA, Taqi MA, Zaidat OO. Vertebral artery stenting for the treatment of bow hunter's syndrome: report of 4 cases. J Stroke Cerebrovasc Dis. 2012; 21:908.e1–908.e5.
Article9. Çevik S, Katar S, Hanımoǧlu H. C1-C2 transverse foramen decompression by anterolateral approach as an alternative treatment in Bow Hunter's syndrome. Asian J Neurosurg. 2018; 13:411–413.
Article10. Velat GJ, Reavey-Cantwell JF, Ulm AJ, Lewis SB. Intraoperative dynamic angiography to detect resolution of Bow Hunter's syndrome: technical case report. Surg Neurol. 2006; 66:420–423. discussion 423.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Rotational Vertebral Artery Compression : Bow Hunter's Syndrome
- Rotational Vertebral Artery Syndrome (Bow Hunter’s Syndrome): A Rare Differential Diagnosis in Patients With Syncope
- A Case of Rotational Vertebral Artery Syndrome after Vertebral Artery Dissection
- Bow Hunter's Stroke Caused by a Severe Facet Hypertrophy of C1-2
- Cervicogenic Vertigo Treated by C1 Transverse Foramen Decompression : A Case Report
