Ann Pediatr Endocrinol Metab.
2019 Dec;24(4):237-242. 10.6065/apem.2019.24.4.237.
Follow-up of infants with congenital hypothyroidism and low total thyroxine/thyroid stimulating hormone on newborn screen
- Affiliations
-
- 1Children's Hospital Alabama, University of Alabama at Birmingham, Birmingham, AL, USA. zachary.hughes@northwestern.edu
- KMID: 2468725
- DOI: http://doi.org/10.6065/apem.2019.24.4.237
Abstract
- PURPOSE
Newborn screening (NBS) methods to detect congenital hypothyroidism (CH) vary regarding whether total thyroxine (T4), thyroid stimulating hormone (TSH), or both are measured. Neonates with low T4 and normal or low TSH (lowT4/TSH) may only be detected by T4-inclusive methods or age-dependent repeat screens. Premature neonates and those with pituitary-hypothalamic disorders frequently manifest lowT4/TSH.
METHODS
This is a retrospective case-study of newborns who were screen-positive for lowT4/TSH in Alabama in 2009-2016 using a combined T4 and TSH method and 2 routine NBS. The clinical, laboratory, and final diagnosis after 3 years were determined.
RESULTS
Over 8 years, 225 infants were referred to our institution for evaluation and treatment of CH. Twelve infants were screen-positive for lowT4/TSH by first or second NBS. Four of the 12 infants had permanent CH (30%): 2 with primary and 2 with central etiologies. One infant with moderately severe central CH was only detected by the routine second NBS. Six of 7 premature infants had elevated TSH on serum confirmation labs consistent with a delay in hypothalamic-pituitary maturation, yet 2 of these patients were later established to have permanent primary CH. While most cases of lowT4/TSH resolved by 3 years of age, several neonates had extended periods of moderate to severe hypothyroxinemia prior to detection and treatment.
CONCLUSION
One third of the infants with lowT4/TSH on NBS in this study had permanent CH. These results emphasize the importance of T4-based assay methods, subsequent (repeat) screens and long-term follow-up in the management of neonates with lowT4/TSH on newborn screen.
Keyword
MeSH Terms
Figure
-
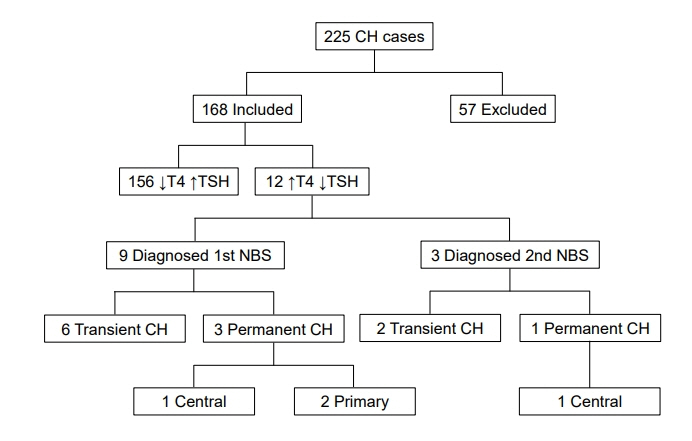
Fig. 1. Patients with congenital hypothyroidism (CH) detected by newborn screen (NBS) in Alabama between 2009 and 2016. T4, total thyroxine; TSH, thyroid stimulating hormone.
Reference
-
References
1. Léger J, Olivieri A, Donaldson M, Torresani T, Krude H, van Vliet G, et al. European Society for Paediatric Endocrinology consensus guidelines on screening, diagnosis, and management of congenital hypothyroidism. J Clin Endocrinol Metab. 2014; 99:363–84.
Article2. Shapira SK, Hinton CF, Held PK, Jones E, Harry Hannon W, Ojodu J. Single newborn screen or routine second screening for primary congenital hypothyroidism. Mol Genet Metab. 2015; 116:125–32.
Article3. Ford GA, Denniston S, Sesser D, Skeels MR, LaFranchi SH. Transient versus permanent congenital hypothyroidism after the age of 3 years in infants detected on the first versus second newborn screening test in Oregon, USA. Horm Res Paediatr. 2016; 86:169–77.
Article4. Jones DE, Hart K, Shapira SK, Murray M, Atkinson-Dunn R, Rohrwasser A. Identification of primary congenital hypothyroidism based on two newborn screens - Utah, 2010-2016. MMWR Morb Mortal Wkly Rep. 2018; 67:782–5.
Article5. Kilberg MJ, Rasooly IR, LaFranchi SH, Bauer AJ, Hawkes CP. Newborn screening in the US may miss mild persistent hypothyroidism. J Pediatr. 2018; 192:204–8.
Article6. Woo HC, Lizarda A, Tucker R, Mitchell ML, Vohr B, Oh W, et al. Congenital hypothyroidism with a delayed thyroidstimulating hormone elevation in very premature infants: incidence and growth and developmental outcomes. J Pediatr. 2011; 158:538–42.
Article7. Zung A, Yehieli A, Blau A, Almashanu S. Characteristics of Delayed thyroid stimulating hormone elevation in neonatal intensive care unit newborns. J Pediatr. 2016; 178:135–40. e1.
Article8. Vigone MC, Caiulo S, Di Frenna M, Ghirardello S, Corbetta C, Mosca F, et al. Evolution of thyroid function in preterm infants detected by screening for congenital hypothyroidism. J Pediatr. 2014; 164:1296–302.
Article9. McGrath N, Hawkes CP, Mayne P, Murphy NP. Optimal timing of repeat newborn screening for congenital hypothyroidism in preterm infants to detect delayed thyroid-stimulating hormone elevation. J Pediatr. 2019; 205:77–82.
Article10. Nebesio TD, McKenna MP, Nabhan ZM, Eugster EA. Newborn screening results in children with central hypothyroidism. J Pediatr. 2010; 156:990–3.
Article11. Zwaveling-Soonawala N, van Trotsenburg AS, Verkerk PH. The severity of congenital hypothyroidism of central origin should not be underestimated. J Clin Endocrinol Metab. 2015; 100:E297–300.
Article12. Connelly KJ, LaFranchi SH. Detection of neonates with mild congenital hypothyroidism (primary) or isolated hyperthyrotropinemia: an increasingly common management dilemma. Expert Rev Endocrinol Metab. 2014; 9:263–71.
Article13. LaFranchi SH. Approach to the diagnosis and treatment of neonatal hypothyroidism. J Clin Endocrinol Metab. 2011; 96:2959–67.
Article14. American Academy of Pediatrics, Rose SR; Section on Endocrinology and Committee on Genetics; American Thyroid Association, Brown RS; Public Health Committee; Lawson Wilkins Pediatric Endocrine Society, Foley T, et al. Update of newborn screening and therapy for congenital hypothyroidism. Pediatrics. 2006; 117:2290–303.
Article15. Schushan-Eisen I, Lazar L, Amitai N, Meyerovitch J. Thyroid functions in healthy infants during the first year of life. J Pediatr. 2016; 170:120–5. e1.
Article16. Wassner AJ, Brown RS. Subclinical hypothyroidism in infancy: to treat or not to treat, that is the question. J Pediatr. 2016; 170:17–9.
Article17. Braslavsky D, Méndez MV, Prieto L, Keselman A, Enacan R, Gruñeiro-Papendieck L, et al. Pilot neonatal screening program for central congenital hypothyroidism: evidence of significant detection. Horm Res Paediatr. 2017; 88:274–80.
Article18. Ahmet A, Lawson ML, Babyn P, Tricco AC. Hypothyroidism in neonates post-iodinated contrast media: a systematic review. Acta Paediatr. 2009; 98:1568–74.
Article19. Barr ML, Chiu HK, Li N, Yeh MW, Rhee CM, Casillas J, et al. Thyroid dysfunction in children exposed to iodinated contrast media. J Clin Endocrinol Metab. 2016; 101:2366–70.
Article20. Cuestas E, Gaido MI, Capra RH. Transient neonatal hyperthyrotropinemia is a risk factor for developing persistent hyperthyrotropinemia in childhood with repercussion on developmental status. Eur J Endocrinol. 2015; 172:483–90.
Article21. Lim HH, Yang SW. Risk factor for pituitary dysfunction in children and adolescents with Rathke's cleft cysts. Korean J Pediatr. 2010; 53:759–65.
Article22. Schoenmakers N, Alatzoglou KS, Chatterjee VK, Dattani MT. Recent advances in central congenital hypothyroidism. J Endocrinol. 2015; 227:R51–71.
Article23. Van den Berghe G, de Zegher F, Lauwers P. Dopamine suppresses pituitary function in infants and children. Crit Care Med. 1994; 22:1747–53.
Article24. Tonyushkina KN, Krug S, Ortiz-Toro T, Mascari T, Karlstrom RO. Low thyroid hormone levels disrupt thyrotrope development. Endocrinology. 2017; 158:2774–82.
Article25. Huang SA, Tu HM, Harney JW, Venihaki M, Butte AJ, Kozakewich HP, et al. Severe hypothyroidism caused by type 3 iodothyronine deiodinase in infantile hemangiomas. N Engl J Med. 2000; 343:185–9.
Article26. Luongo C, Trivisano L, Alfano F, Salvatore D. Type 3 deiodinase and consumptive hypothyroidism: a common mechanism for a rare disease. Front Endocrinol (Lausanne). 2013; 4:115.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Thyroxine Binding Globulin Deficiency with Hypothyroidism
- Thyroid dysfunction in very low birth weight preterm infants
- Screening and management of thyroid dysfunction in preterm infants
- A Case of Neonatal Dual Ectopic Thyroid Glands with Congenital Hypothyroidism
- Factors Distinguishing between Transient and Permanent Hypothyroidism in Patients Diagnosed as Congenital Hypothyroidism by Newborn Screening
