Effect of Operator Volume on In-Hospital Outcomes Following Primary Percutaneous Coronary Intervention for ST-Elevation Myocardial Infarction: Based on the 2014 Cohort of Korean Percutaneous Coronary Intervention (K-PCI) Registry
- Affiliations
-
- 1Division of Cardiovascular, Department of Internal Medicine, Yeungnam University Medical Center, Yeungnam University College of Medicine, Daegu, Korea. pjs@med.yu.ac.kr
- 2Department of Preventive Medicine, Chungbuk National University College of Medicine, Cheongju, Korea.
- 3Division of Cardiology, National Health Insurance Service (NHIS) Ilsan Hospital, Goyang, Korea.
- 4Heart Center, Konyang University Hospital, Daejeon, Korea.
- 5Department of Cardiovascular Medicine, Regional Cardiocerebrovascular Center, Wonkwang University Hospital, Iksan, Korea.
- 6Department of Internal Medicine, Pusan National University Hospital, Busan, Korea.
- 7Department of Cardiology, Myongji Hospital, Goyang, Korea.
- 8Division of Cardiology, Department of Internal Medicine, Chosun University College of Medicine, Gwangju, Korea.
- 9Department of Cardiology, Inje University Busan Paik Hospital, Busan, Korea.
- 10Division of Cardiovascular, Department of Internal Medicine, Good Morning Hospital, Pyeongtaek, Korea.
- 11Department of Internal Medicine, Chungbuk National University, Cheongju, Korea. drcorazon@hanmail.net
- KMID: 2468039
- DOI: http://doi.org/10.4070/kcj.2019.0206
Abstract
- BACKGROUND AND OBJECTIVES
The relationship between operator volume and outcomes of percutaneous coronary intervention (PCI) in patients with ST-elevation myocardial infarction (STEMI) has not been fully investigated. We aimed to investigate the relationship between operator PCI volume and in-hospital outcomes after primary PCI for STEMI.
METHODS
Among the total of 44,967 consecutive cases of PCI enrolled in the Korean nationwide, retrospective registry (K-PCI registry), 8,282 patients treated with PCI for STEMI by 373 operators were analyzed. PCI volumes above the 75th percentile (>30 cases/year), between the 75th and 25th percentile (10-30 cases/year), and below the 25th percentile (<10 cases/year) were defined as high, moderate, and low-volume operators, respectively. In-hospital outcomes including mortality, non-fatal myocardial infarction (MI), stent thrombosis, stroke, and urgent repeat PCI were analyzed.
RESULTS
The average number of primary PCI cases performed by 373 operators was 22.2 in a year. In-hospital mortality after PCI for STEMI was 571 cases (6.9%). In-hospital outcomes by operator volume showed no significant differences in the death rate, cardiac death, non-fatal MI, and stent thrombosis. However, the rate of urgent repeat PCI tended to be lower in the high-volume operator (0.6%) than in the moderate-(0.7%)/low-(1.5%) volume operator groups (p=0.095). The adjusted odds ratios for adverse in-hospital outcomes were similar in the 3 groups. Multivariate analysis also showed that operator volume was not a predictor for adverse in-hospital outcomes.
CONCLUSIONS
In-hospital outcomes after primary PCI for STEMI were not associated with operator volume in the K-PCI registry.
Keyword
MeSH Terms
Figure
-

Figure 1 The geographic pattern of operator volume showed that the mean number of primary percutaneous coronary intervention cases was significantly higher in Honam province than other provinces. PCI = percutaneous coronary intervention.
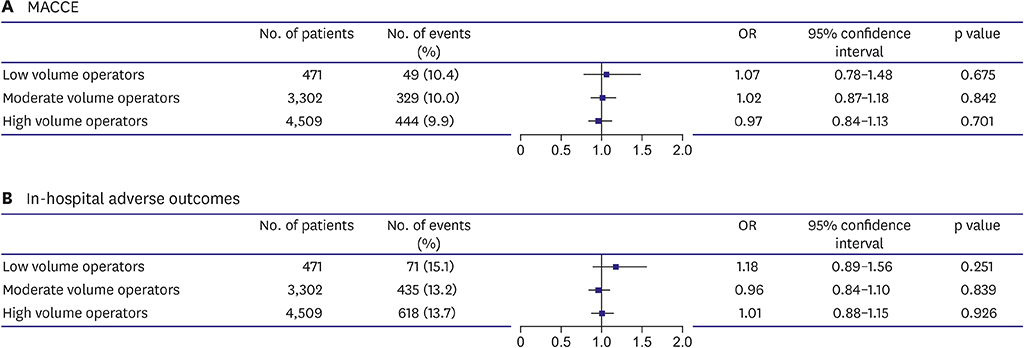
Figure 2 (A) The adjusted OR for MACCE according to operator volume. (B) The adjusted OR for adverse in-hospital outcomes according to operator volume. We adjusted confounding factor, such as age, sex, hypertension, diabetes, family history of premature coronary artery disease, prior percutaneous coronary intervention, and renal failure. MACCE = major adverse cardiovascular and cerebrovascular event; OR = odds ratio.
Cited by 3 articles
-
Impact of Hospital Volume of Percutaneous Coronary Intervention (PCI) on In-Hospital Outcomes in Patients with Acute Myocardial Infarction: Based on the 2014 Cohort of the Korean Percutaneous Coronary Intervention (K-PCI) Registry
Byong-Kyu Kim, Deuk-Young Nah, Kang Un Choi, Jun-Ho Bae, Moo-Yong Rhee, Jae-Sik Jang, Keon-Woong Moon, Jun-Hee Lee, Hee-Yeol Kim, Seung-Ho Kang, Woo hyuk Song, Seung Uk Lee, Byung-Ju Shim, Hangjae Chung, Min Su Hyon
Korean Circ J. 2020;50(11):1026-1036. doi: 10.4070/kcj.2020.0172.The Operator Volume of Primary Percutaneous Coronary Intervention for ST Segment Elevation Myocardial Infarction Does Not Guarantee Its Quality in Korea
Chang-Hwan Yoon
Korean Circ J. 2020;50(2):145-147. doi: 10.4070/kcj.2019.0389.Implementation of National Health Policy for the Prevention and Control of Cardiovascular Disease in South Korea: Regional-Local Cardio-Cerebrovascular Center and Nationwide Registry
Ju Mee Wang, Byung Ok Kim, Jang-Whan Bae, Dong-Jin Oh
Korean Circ J. 2021;51(5):383-398. doi: 10.4070/kcj.2021.0001.
Reference
-
1. Hannan EL, Wu C, Walford G, et al. Volume-outcome relationships for percutaneous coronary interventions in the stent era. Circulation. 2005; 112:1171–1179.
Article2. Moscucci M, Share D, Smith D, et al. Relationship between operator volume and adverse outcome in contemporary percutaneous coronary intervention practice: an analysis of a quality-controlled multicenter percutaneous coronary intervention clinical database. J Am Coll Cardiol. 2005; 46:625–632.
Article3. Badheka AO, Patel NJ, Grover P, et al. Impact of annual operator and institutional volume on percutaneous coronary intervention outcomes: a 5-year United States experience (2005–2009). Circulation. 2014; 130:1392–1406.4. Fanaroff AC, Zakroysky P, Dai D, et al. Outcomes of PCI in relation to procedural characteristics and operator volumes in the United States. J Am Coll Cardiol. 2017; 69:2913–2924.5. Jang JS, Han KR, Moon KW, et al. The current status of percutaneous coronary intervention in Korea: based on year 2014 cohort of Korean percutaneous coronary intervention (K-PCI) registry. Korean Circ J. 2017; 47:328–340.
Article6. Writing Committee Members. Harold JG, Bass TA, et al. ACCF/AHA/SCAI 2013 update of the clinical competence statement on coronary artery interventional procedures: a report of the American College of Cardiology Foundation/American Heart Association/American College of Physicians task force on clinical competence and training (writing committee to revise the 2007 clinical competence statement on cardiac interventional procedures). Catheter Cardiovasc Interv. 2013; 82:E69–111.7. Windecker S, Kolh P, Alfonso F, et al. 2014 ESC/EACTS guidelines on myocardial revascularization. EuroIntervention. 2015; 10:1024–1094.
Article8. Inohara T, Kohsaka S, Yamaji K, et al. Impact of institutional and operator volume on short-term outcomes of percutaneous coronary intervention: a report from the Japanese nationwide registry. JACC Cardiovasc Interv. 2017; 10:918–927.9. Hulme W, Sperrin M, Curzen N, et al. Operator volume is not associated with mortality following percutaneous coronary intervention: insights from the British Cardiovascular Intervention Society registry. Eur Heart J. 2018; 39:1623–1634.
Article10. Ibanez B, James S, Agewall S, et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018; 39:119–177.11. Levine GN, Bates ER, Blankenship JC, et al. 2015 ACC/AHA/SCAI focused update on primary percutaneous coronary intervention for patients with ST-elevation myocardial infarction: an update of the 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention and the 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction. J Am Coll Cardiol. 2016; 67:1235–1250.12. Cutlip DE, Windecker S, Mehran R, et al. Clinical end points in coronary stent trials: a case for standardized definitions. Circulation. 2007; 115:2344–2351.13. Thygesen K, Alpert JS, Jaffe AS, et al. Fourth universal definition of myocardial infarction (2018). J Am Coll Cardiol. 2018; 72:2231–2264.
Article14. Srinivas VS, Hailpern SM, Koss E, Monrad ES, Alderman MH. Effect of physician volume on the relationship between hospital volume and mortality during primary angioplasty. J Am Coll Cardiol. 2009; 53:574–579.
Article15. Jolly SS, Yusuf S, Cairns J, et al. Radial versus femoral access for coronary angiography and intervention in patients with acute coronary syndromes (RIVAL): a randomised, parallel group, multicentre trial. Lancet. 2011; 377:1409–1420.
Article16. Zhang J, Gao X, Kan J, et al. Intravascular ultrasound versus angiography-guided drug-eluting stent implantation: the ULTIMATE trial. J Am Coll Cardiol. 2018; 72:3126–3137.17. Hong SJ, Kim BK, Shin DH, et al. Effect of intravascular ultrasound-guided vs angiography-guided everolimus-eluting stent implantation: the IVUS-XPL randomized clinical trial. JAMA. 2015; 314:2155–2163.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Current Status of Coronary Intervention in Patients with ST-Segment Elevation Myocardial Infarction and Multivessel Coronary Artery Disease
- Consecutive Multivessel Myocardial Infarction during Primary Percutaneous Coronary Intervention
- The Operator Volume of Primary Percutaneous Coronary Intervention for ST Segment Elevation Myocardial Infarction Does Not Guarantee Its Quality in Korea
- Impact of Hospital Volume of Percutaneous Coronary Intervention (PCI) on In-Hospital Outcomes in Patients with Acute Myocardial Infarction: Based on the 2014 Cohort of the Korean Percutaneous Coronary Intervention (K-PCI) Registry
- The Prognostic Impact of Hypertriglyceridemia and Abdominal Obesity in Acute Myocardial Infarction Patients Underwent Percutaneous Coronary Intervention
