Incidence and Clinical Significance of Positional Downbeat Nystagmus in Posterior Canal Benign Paroxysmal Positional Vertigo
- Affiliations
-
- 1Department of Neurology, Pusan National University School of Medicine, Research Institute for Convergence of Biomedical Science and Technology, Pusan National University Yangsan Hospital, Yangsan, Korea. rachelbolan@hanmail.net
- 2Research Administration Team, Seoul National University Bundang Hospital, Seongnam, Korea.
- 3Department of Neurology, Pusan National University Hospital, Pusan National University School of Medicine and Biomedical Research Institute, Busan, Korea.
- KMID: 2467726
- DOI: http://doi.org/10.3988/jcn.2019.15.2.143
Abstract
- BACKGROUND AND PURPOSE
The aim of this study was to determine the incidence and clinical significance of positional downbeat nystagmus (pDBN) after treatment of posterior canal (PC) benign paroxysmal positional vertigo (BPPV).
METHODS
We recruited 77 patients with a diagnosis of PC BPPV, and assessed the presence of pDBN during follow-up positional tests after performing the Epley maneuver.
RESULTS
An immediate response to the Epley maneuver was exhibited by 57 of the 77 patients, with resolution of their positional torsional upbeat nystagmus (pT-UBN). Twenty-two (39%) of them exhibited pDBN during follow-up tests performed 1 hour later. The latency and duration of pDBN were 3.2±2.0 and 12.0±10.0 s (mean±SD), respectively. The maximum slowphase velocity of pDBN was 5.1±2.5 degrees, and ranged from 2.0 to 12.2 degrees. A torsional component was also observed in six patients. The patients with pDBN were much more likely to develop a typical form of PC BPPV again at a 1-week follow-up (5/22, 23%) compared to those without pDBN (1/31, 3%; p=0.036). pDBN disappeared in all patients within 6 months.
CONCLUSIONS
Our study found transient pDBN in 40% of patients with PC BPPV after the immediate resolution of positional vertigo and pT-UBN. pDBN may be attributed to residual debris in the distal portion of the PC, which can move toward the ampulla producing an ampullopetal flow of endolymph during positioning.
Keyword
MeSH Terms
Figure
-
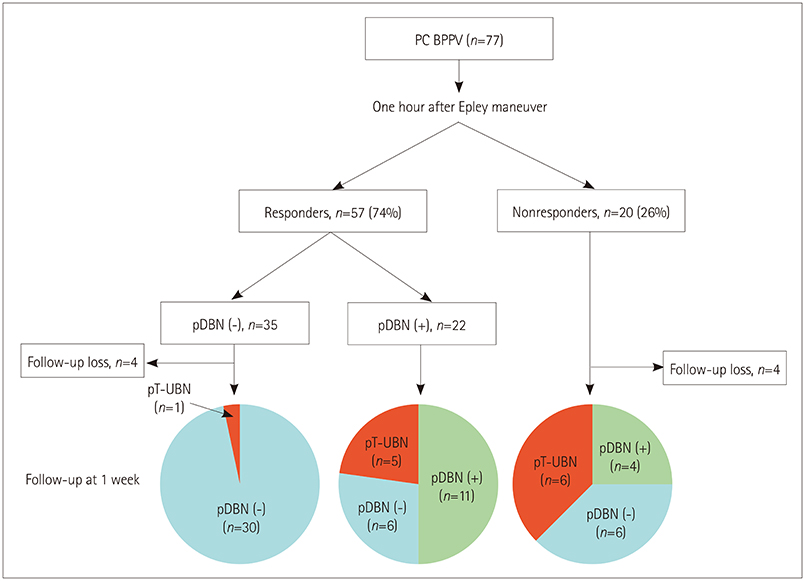
Fig. 1 Treatment outcome, incidence of pDBN, and 1-week follow-up results in patients with PC BPPV. The responders were those patients with resolution of pT-UBN in follow-up tests performed 1 hour after the Epley maneuver. BPPV: benign paroxysmal positional vertigo, PC: posterior canal, pDBN: positional downbeat nystagmus, pT-UBN: positional vertigo and torsional upbeat nystagmus.
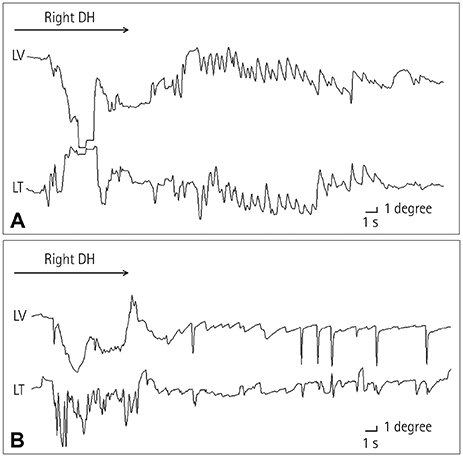
Fig. 2 Recording of positional nystagmus in a patient with right-side posterior canal benign paroxysmal positional vertigo. A: Initially, the right-side DH maneuver induced upbeat and CW torsional nystagmus. B: One hour after receiving the Epley maneuver, downbeat nystagmus with a small counterclockwise torsional component was observed during the right-side DH maneuver. Upward deflection indicates upward and CW eye motion from the patient's perspective. CW: clockwise, DH: Dix-Hallpike, LT: torsional position of the left eye, LV: vertical position of the left eye.
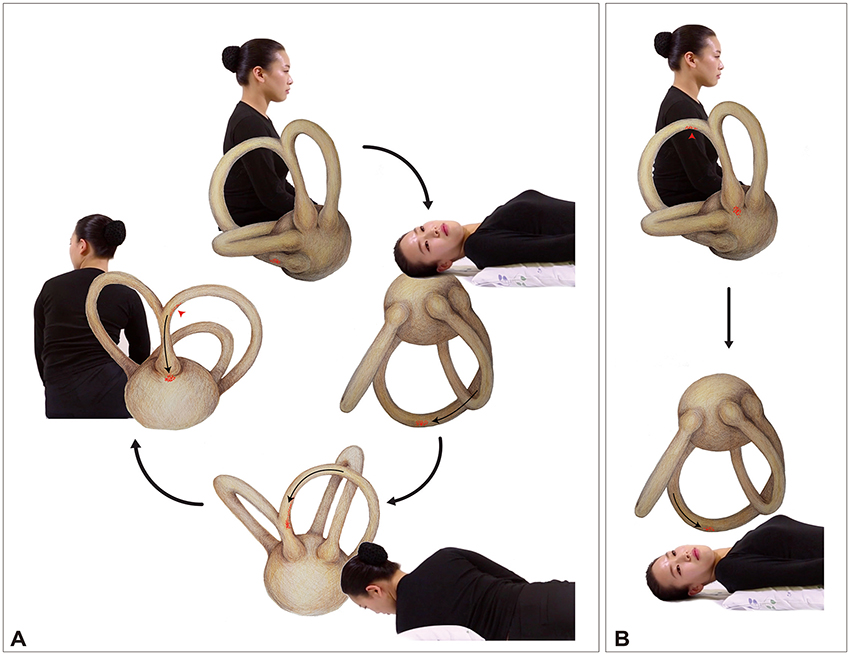
Fig. 3 Positional downbeat nystagmus due to canalolithiasis in the nonampullary arm of the PC. A: During the Epley maneuver, some otoconial debris can remain in the nonampullary arm of the PC near the common crus (red arrowhead). B: When a patient lies down to assume the head-hanging position, the residual debris in the PC (red arrowhead) moves toward the ampulla, producing an ampullopetal flow of endolymph and downbeat nystagmus. PC: posterior canal.
Reference
-
1. Macdonald NK, Kaski D, Saman Y, Al-Shaikh Sulaiman A, Anwer A, Bamiou DE. Central positional nystagmus: a systematic literature review. Front Neurol. 2017; 8:141.
Article2. Choi JY, Kim JH, Kim HJ, Glasauer S, Kim JS. Central paroxysmal positional nystagmus: characteristics and possible mechanisms. Neurology. 2015; 84:2238–2246.
Article3. Brandt T. Positional and positioning vertigo and nystagmus. J Neurol Sci. 1990; 95:3–28.
Article4. Lee JY, Lee WW, Kim JS, Kim HJ, Kim JK, Jeon BS. Perverted head-shaking and positional downbeat nystagmus in patients with multiple system atrophy. Mov Disord. 2009; 24:1290–1295.
Article5. Bertholon P, Bronstein AM, Davies RA, Rudge P, Thilo KV. Positional down beating nystagmus in 50 patients: cerebellar disorders and possible anterior semicircular canalithiasis. J Neurol Neurosurg Psychiatry. 2002; 72:366–372.
Article6. Ogawa Y, Suzuki M, Otsuka K, Shimizu S, Inagaki T, Hayashi M, et al. Positional and positioning down-beating nystagmus without central nervous system findings. Auris Nasus Larynx. 2009; 36:698–701.
Article7. Kim JS, Zee DS. Clinical practice. benign paroxysmal positional vertigo. N Engl J Med. 2014; 370:1138–1147.8. Imai T, Takeda N, Ito M, Nakamae K, Sakae H, Fujioka H, et al. Three-dimensional analysis of benign paroxysmal positional nystagmus in a patient with anterior semicircular canal variant. Otol Neurotol. 2006; 27:362–366.
Article9. Yacovino DA, Hain TC, Gualtieri F. New therapeutic maneuver for anterior canal benign paroxysmal positional vertigo. J Neurol. 2009; 256:1851–1855.
Article10. Anagnostou E, Kouzi I, Spengos K. Diagnosis and treatment of anterior-canal benign paroxysmal positional vertigo: a systematic review. J Clin Neurol. 2015; 11:262–267.
Article11. Vannucchi P, Pecci R, Giannoni B. Posterior semicircular canal benign paroxysmal positional vertigo presenting with torsional downbeating nystagmus: an apogeotropic variant. Int J Otolaryngol. 2012; 2012:413603.
Article12. Vannucchi P, Pecci R, Giannoni B, Di Giustino F, Santimone R, Mengucci A. Apogeotropic posterior semicircular canal benign paroxysmal positional vertigo: some clinical and therapeutic considerations. Audiol Res. 2015; 5:130.
Article13. Califano L, Salafia F, Mazzone S, Melillo MG, Califano M. Anterior canal BPPV and apogeotropic posterior canal BPPV: two rare forms of vertical canalolithiasis. Acta Otorhinolaryngol Ital. 2014; 34:189–197.14. Büki B, Mandalà M, Nuti D. Typical and atypical benign paroxysmal positional vertigo: literature review and new theoretical considerations. J Vestib Res. 2014; 24:415–423.
Article15. Cambi J, Astore S, Mandalà M, Trabalzini F, Nuti D. Natural course of positional down-beating nystagmus of peripheral origin. J Neurol. 2013; 260:1489–1496.
Article16. von Brevern M, Bertholon P, Brandt T, Fife T, Imai T, Nuti D, et al. Benign paroxysmal positional vertigo: diagnostic criteria. J Vestib Res. 2015; 25:105–117.
Article17. Kanebayashi H, Suzuki M, Ogawa Y. Measurement of helical angle of the human semicircular canals using rapid-prototyped inner ear model. Equilib Res. 2008; 67:294–300.
Article18. Giommetti G, Lapenna R, Panichi R, Mobaraki PD, Longari F, Ricci G, et al. Residual dizziness after successful repositioning maneuver for idiopathic benign paroxysmal positional vertigo: a review. Audiol Res. 2017; 7:178.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Positional Dizziness and Vertigo without Nystagmus and Orthostatic Hypotension
- An Atypical Case of Benign Paroxysmal Positional Vertigo of the Anterior Semicircular Canal
- Various Nystagmus Patterns and Their Clinical Significance in Benign Paroxysmal Positional Vertigo of Anterior Semicircular Canal
- Positional Vertigo Showing Direction-Changing Positional Nystagmus after Chronic Otitis Media Surgery: Is It Benign Paroxysmal Positional Vertigo?
- The Head-Bending Test in Posterior Semicircular Canal Benign Paroxysmal Positional Vertigo
