Communicating Bronchopulmonary Foregut Malformation Type III with Pulmonary Sequestration Diagnosed in a Newborn: A Case Report
- Affiliations
-
- 1Department of Pediatrics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. sein.sung@samsung.com
- 2Department of Pediatrics, Korea University Guro Hospital, Korea University School of Medicine, Seoul, Korea.
- 3Division of Thoracic Surgery, Department of Thoracic Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2466643
- DOI: http://doi.org/10.5385/nm.2019.26.4.223
Abstract
- Communicating bronchopulmonary foregut malformation (CBPFM) is a communication between the respiratory and gastrointestinal tracts that can be difficult to differentiate from pulmonary sequestration or H-type tracheoesophageal fistula (TEF) because of the similarities in clinical features. A female neonate born at full term had been experiencing respiratory difficulty during feeding from the third day of life. The esophagography performed to rule out H-type TEF revealed that the esophageal bronchus directly communicated with the left lower lobe (LLL) of the lung. Lobectomy of the LLL, fistulectomy of the esophagobronchial fistula, and primary repair of the esophagus were performed. Finally, CBPFM type III with pulmonary sequestration was confirmed on the basis of the postoperative histopathological finding. We report the first newborn case of CBPFM type III with pulmonary sequestration in Korea.
MeSH Terms
Figure
-

Figure 1. Chest radiograph after gastric tube insertion (at birth). Increased opacity is found involving the left lower lung field (solid arrow). The cardiac size is borderline. A feeding tube is placed with its tip on the stomach, which is located more medial than usual and associated with visible small bowel gases in the right abdomen, suspected to be gastrointestinal malrotation.
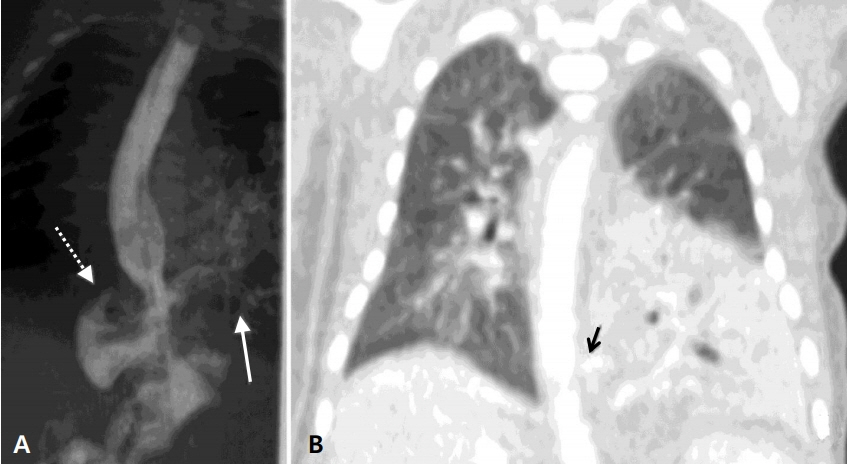
Figure 2. (A) Esophagogram. The esophagus is directly communicating with the bronchus from the left lower lobe of the lung (solid arrow), combined with a suspected right gastric diverticulum (dotted arrow). (B) Chest computed tomography scans (coronal view). The left lower lobe, which contains atelectasis and consolidation, is supplied by the aberrant artery arising from the celiac trunk. A lesion suspected to be a fistula (solid arrow) is found between the esophagus and the bronchus.
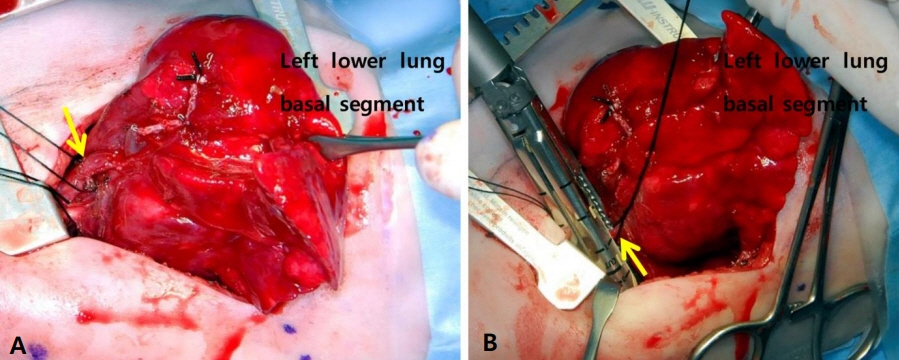
Figure 3. (A) Intraoperative demonstration of the anatomy. The feeding artery (solid arrow) from the celiac trunk is depicted. (B) Intraoperative demonstration of the anatomy. The fistula (solid arrow) connecting the esophagus to the bronchus is shown.
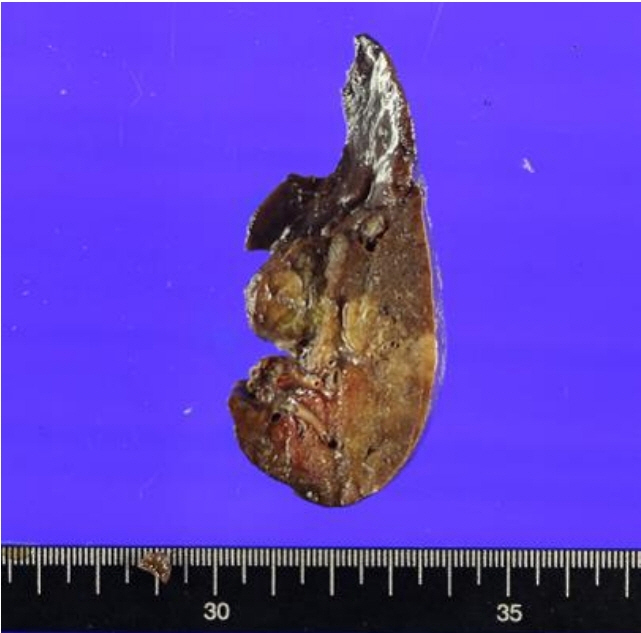
Figure 4. Gross surgical specimen of the resected left lower lobe. The left lower lobe tissue measures 8×5×3 cm. The gross finding shows bronchiectasis or a dilatated cystic area.
Reference
-
1. Bokka S, Jaiswal AA, Behera BK, Mohanty MK, Khare MK, Garg AK. Esophageal lung: a rare type of communicating bronchopulmonary foregut malformation, case report with review of literature. J Indian Assoc Pediatr Surg. 2015; 20:92–4.2. Sugandhi N, Sharma P, Agarwala S, Kabra SK, Gupta AK, Gupta DK. Esophageal lung: presentation, management, and review of literature. J Pediatr Surg. 2011; 46:1634–7.3. Verma A, Mohan S, Kathuria M, Baijal SS. Esophageal bronchus: case report and review of the literature. Acta Radiol. 2008; 49:138–41.4. Pimpalwar AP, Hassan SF. Esophageal bronchus in an infant: a rare cause of recurrent pneumonia. J Pediatr Surg. 2012; 47:e5. –8.5. Chung JH, Lim GY, Kim SY. Esophageal lung diagnosed following the primary repair of esophageal atresia with tracheo-esophageal fistula in a neonate. Surg Radiol Anat. 2014; 36:397–400.6. Kim CW, Kim DH. Single-incision video-assisted thoracic surgery lobectomy in the treatment of adult communicating bronchopulmonary foregut malformation with large aberrant artery. J Thorac Dis. 2016; 8:E148–51.7. Park T, Jung K, Kim HY, Jung SE, Park KW. Thoracoscopic management of a communicating bronchopulmonary foregut malformation in a 23-month-old child. J Pediatr Surg. 2012; 47:e21. –3.8. Eom DW, Kang GH, Kim JW, Ryu DS. Unusual bronchopulmonary foregut malformation associated with pericardial defect: bronchogenic cyst communicating with tubular esophageal duplication. J Korean Med Sci. 2007; 22:564–7.9. Kim CY, Goo HW, Kim HJ, Choi SJ, Cho YS, Lee JH, et al. Communicating bronchopulmonary foregut malformation: a case report. J Korean Radiol Soc. 2000; 43:59–61.10. Rathi V, Deshpande S, Nazim A, Domkundwar S. Esophageal lung: a rare case of communicating bronchopulmonary foregut malformation. Indian J Basic Appl Med Res. 2017; 6:450–4.11. Ren H, Duan L, Zhao B, Wu X, Zhang H, Liu C. Diagnosis and treatment of communicating bronchopulmonary foregut malformation: report of two cases and review of the literature. Medicine (Baltimore). 2017; 96:e6307.12. Lacina S, Townley R, Radecki L, Stockinger F, Wyngaarden M. Esophageal lung with cardiac abnormalities. Chest. 1981; 79:468–70.13. Heithoff KB, Sane SM, Williams HJ, Jarvis CJ, Carter J, Kane P, et al. Bronchopulmonary foregut malformations: a unifying etiological concept. AJR Am J Roentgenol. 1976; 126:46–55.14. Hanna EA. Broncho-esophageal fistula with total sequestration of the right lung. Ann Surg. 1964; 159:599–603.15. Leithiser RE Jr, Capitanio MA, Macpherson RI, Wood BP. "Communicating" bronchopulmonary foregut malformations. AJR Am J Roentgenol. 1986; 146:227–31.16. Srikanth MS, Ford EG, Stanley P, Mahour GH. Communicating bronchopulmonary foregut malformations: classification and embryogenesis. J Pediatr Surg. 1992; 27:732–6.17. Gerle RD, Jaretzki A 3rd, Ashley CA, Berne AS. Congenital bronchopulmonary-foregut malformation: pulmonary sequestration communicating with the gastrointestinal tract. N Engl J Med. 1968; 278:1413–9.18. Elumalai G, Arjet H. “Tracheoesophageal fistula” embryological basis and its clinical significance. Int J Dev Biol. 2016; 100:43414–9.19. Halasz NA, Lindskog GE, Liebow AA. Esophago-bronchial fistula and bronchopulmonary sequestration: report of a case and review of the literature. Ann Surg. 1962; 155:215–20.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Complex Bronchopulmonary Foregut Malformation: Extralobar Pulmonary Sequestration Communicating with an Esophageal Duplication Cyst: A Case Report
- Extralobar pulmonary sequestration with an associated cyst of mixed bronchogenic and esophageal type--a case report
- A Communicating Bronchopulmonary Foregut Malformation Associated with Absence of the Left Pericardium: A case report
- Mixed Form of Congenital Cystic Adenomatoid Malformation and Extralobar Bronchopulmonary Sequestration: A Case Report
- Congenital Cystic Adenomatoid Malformation Associated with Extralobar Pulmonary Sequestration: A case report
