Postoperative Evaluation after Anterior Cruciate Ligament Reconstruction: Measurements and Abnormalities on Radiographic and CT Imaging
- Affiliations
-
- 1Department of Radiology, Nowon Eulji Medical Center, Eulji University, Seoul 01830, Korea. cys0128@eulji.ac.kr
- 2Department of Orthopedic Surgery, Nowon Eulji Medical Center, Eulji University, Seoul 01830, Korea.
- KMID: 2466289
- DOI: http://doi.org/10.3348/kjr.2016.17.6.919
Abstract
- Reconstruction of a ruptured anterior cruciate ligament (ACL) is a well-established procedure for repair of ACL injury. Despite improvement of surgical and rehabilitation techniques over the past decades, up to 25% of patients still fail to regain satisfactory function after an ACL reconstruction. With development of CT imaging techniques for reducing metal artifacts, multi-planar reconstruction, and three-dimensional reconstruction, early post-operative imaging is increasingly being used to provide immediate feedback to surgeons regarding tunnel positioning, fixation, and device placement. Early post-operative radiography and CT imaging are easy to perform and serve as the baseline examinations for future reference.
Keyword
MeSH Terms
Figure
-
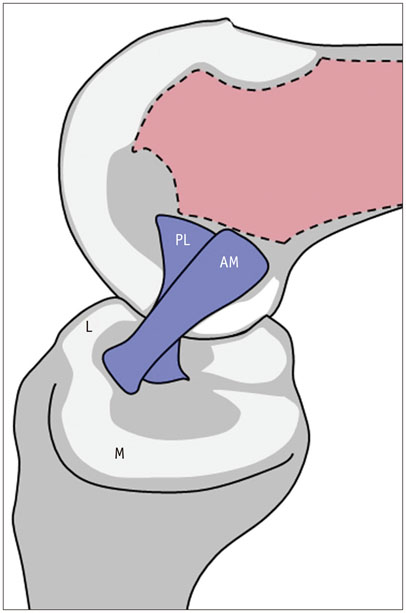
Fig. 1 Schematic drawing of ACL bundles in flexed knee. Anteromedial (AM) bundle includes fascicles attached to proximal part of femoral attachment site and to anteromedial aspect of tibial attachment. Posterolateral (PL) bundle consists of fascicles attached to femur distally and to tibia posterolaterally. If knee is extended, PL bundle is taut and has appearance of being flat and broad. On contrary, when knee is flexed, AM bundle becomes taut. ACL = anterior cruciate ligament, L = lateral, M = medial
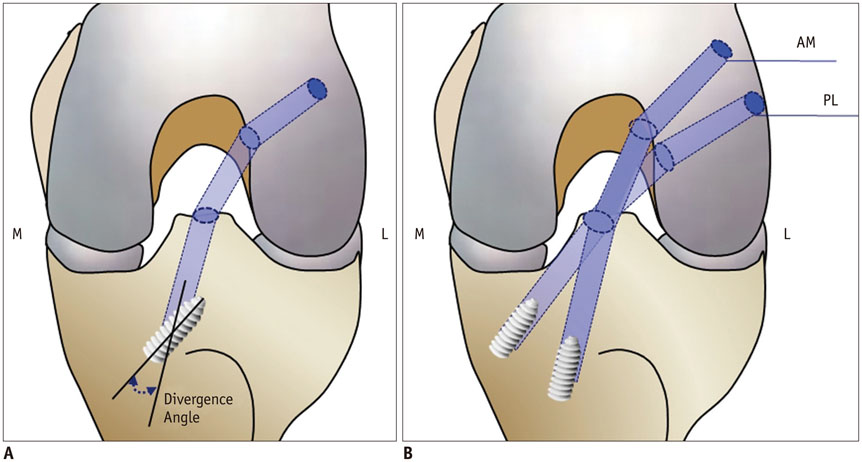
Fig. 2 Illustrations of anteroposterior view of knee showing technique for single bundle (A) and double bundle reconstruction (B) of ACL. ACL = anterior cruciate ligament, AM = anteromedial bundle, L = lateral, M = medial, PL = posterolateral bundle

Fig. 3 Tunnel position after double-bundle ACL reconstruction reflects natural course of two ACL bundles. A. Anteroposterior radiograph showing greater proximal and anterior course of anteromedial (AM) graft (1-o'clock), as compared to posterolateral (PL) graft (2-o'clock) on lateral femoral condyle. B. On oblique radiograph, AM bundle tunnel shows more anterior course than PL bundle tunnel. ACL = anterior cruciate ligament
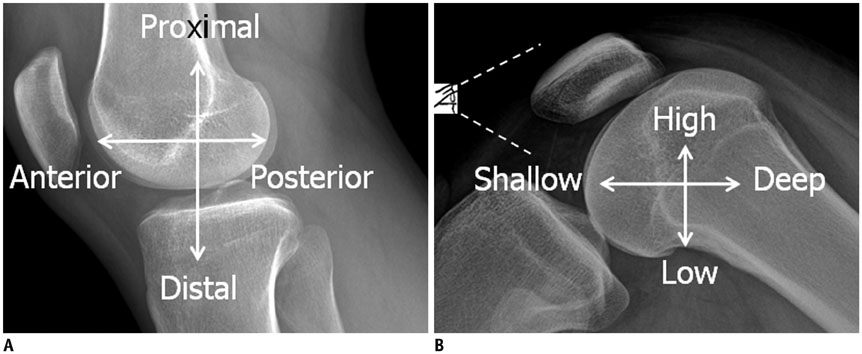
Fig. 4 Terms and directions used in anatomy and radiology (A) and terms and directions used in surgery (B). drawing of eye in (B) represents view in surgery.
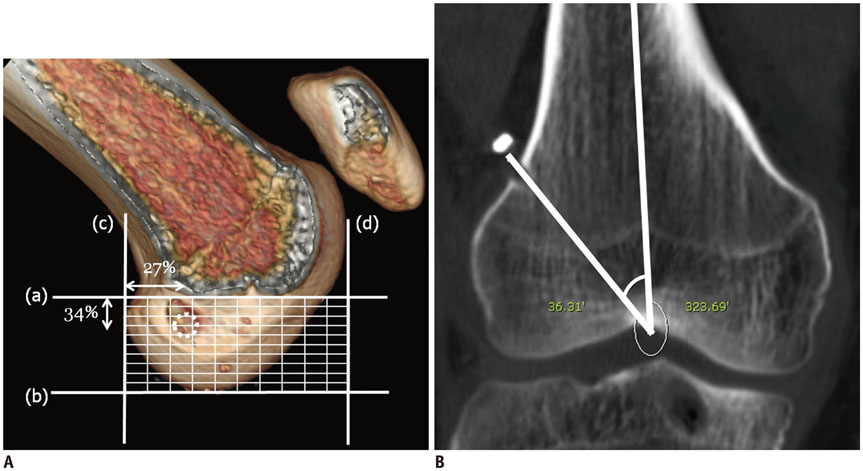
Fig. 5 Normal femoral tunnel position. A. Use of Bernhard and Hertel grid to assess femoral tunnel placement. a = Blumensaat's line: tangent to roof of intercondylar notch, b = Parallel to Blumensaat's line and tangent to inferior border of condyle, c = Perpendicular to Blumensaat's line, at intersection of tangent line with deep border of lateral femoral condyle, d = Perpendicular to Blumensaat's line, at intersection of tangent line with shallow border of lateral femoral condyle. Dotted circle = ideal location, 27% deep-shallow and 34% high-low. B. Angle measurement of femoral tunnel to femur on coronal CT image using picture archiving and communication system software.
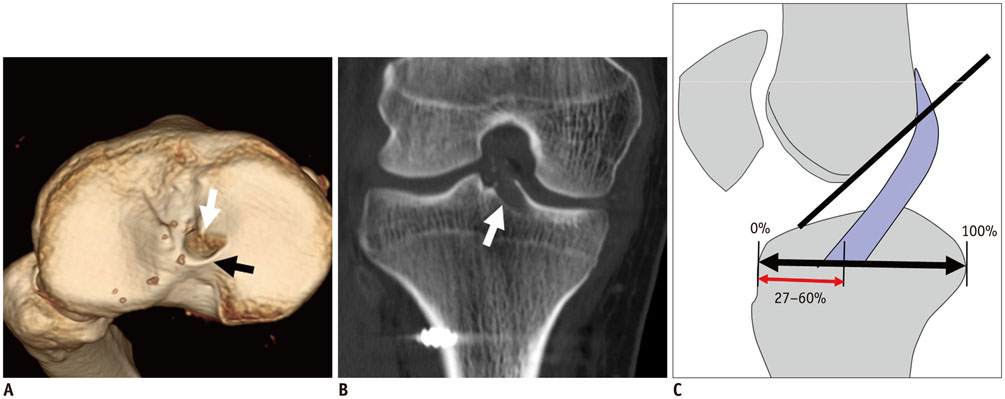
Fig. 6 Normal tibial tunnel position. A. Tibial tunnel (white arrow) is placed at site of tibial footprint; black arrow indicates tibial spine. B. Tibial tunnel (arrow) enters intercondylar notch, in between tibial spines on coronal CT. C. Schematic drawing of lateral view of knee shows intercondylar portion of graft is oriented taut and parallel to or steeper than Blumensaat's line (black line), and entire tunnel is positioned posterior to line extended along Blumensaat's line. Anterior-posterior position of tibial tunnel as ratio is also depicted. Most anterior vertical line indicates 0% and most posterior vertical line, 100% on Amis and Jakob line (black double arrows), respectively. Position of center of ACL tibial insertion (red double arrows) should lie between 27 and 60% along Amis and Jakob line. ACL = anterior cruciate ligament
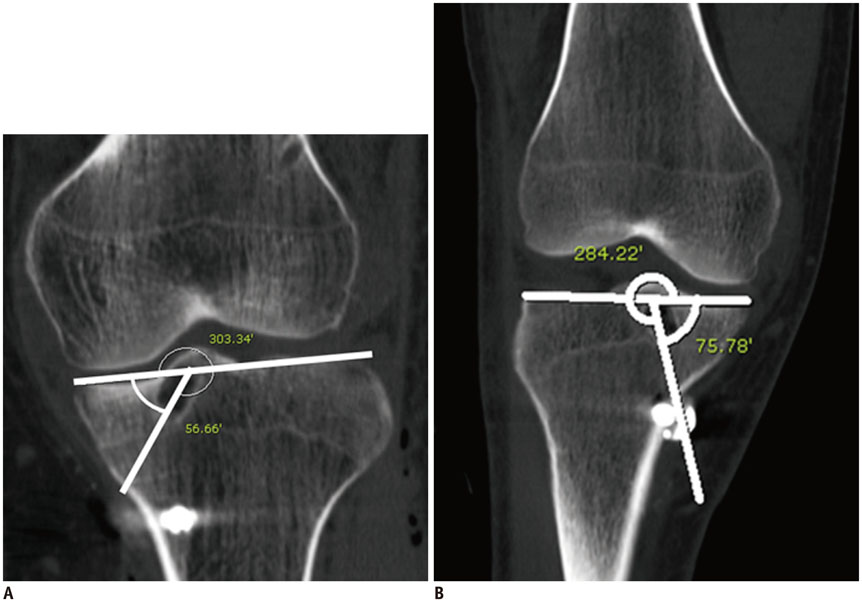
Fig. 7 Angular measurement of tibial tunnel. A. Angle of tibial tunnel with transtibial technique. Angle should not exceed 72°. B. Example of too steep tibial tunnel. Tibial tunnel angle of ≥ 72° is associated with greater loss of flexion and anterior laxity. In this case, angle of tibial tunnel was 75°.

Fig. 8 Normal femoral and tibial tunnels on multiplanar reformat CT images. Oblique coronal multiplanar reformat images aligned along axes of femoral (A) and tibial (B) tunnels clearly demonstrate entire course and width (double arrows) of both tunnels with parallel walls.
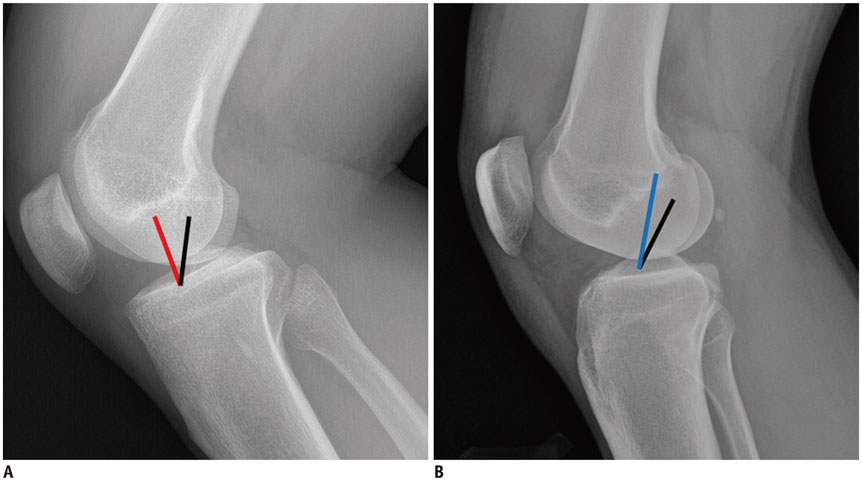
Fig. 9 Schematic drawing of kinematics of graft on flexion (A) and extension (B). Red line demonstrates taut graft in too shallow and too high placed tunnels. If tunnel placement is too high (blue line), graft will be over stretched in extension and may reduce range of motion. Optimal graft placement is indicated with black lines.
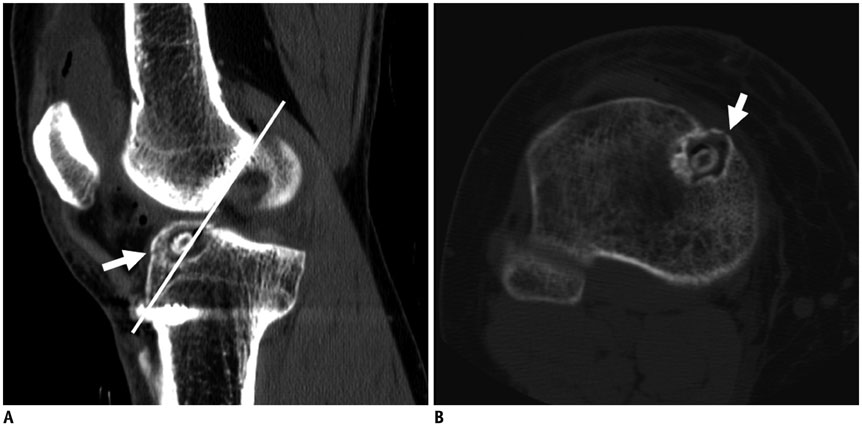
Fig. 10 Example of tibial tunnel positioned too anteriorly. Sagittal CT image reveals tibial tunnel is drilled anterior to Blumensaat's line (white line). Greater anterior placement of tibial tunnel will cause impingement of graft during extension. Note fracture (arrows) in roof of tibial tunnel on sagittal (A) and axial (B) images.

Fig. 11 Migration of button style extra-cortical fixation device. Images obtained immediately (A) and 6 months after surgery (B) show mild sliding of EndoButton fixation device into femoral tunnel (arrows).
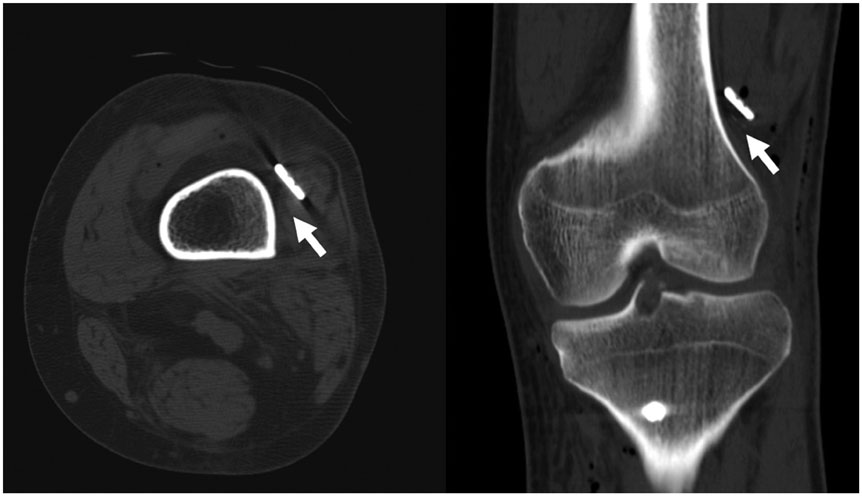
Fig. 12 Gap between fixation device and bone cortex. On axial and coronal post-operative CT scans, gap is seen (arrows) between cortex and fixation device, caused by tissue interposition

Fig. 13 Migration of bioabsorbable interference screws. Compared to that seen on radiograph obtained immediately after surgery (A), tibial fixation screw (arrow) can be seen protruding into anterior knee on radiograph obtained on 6-month follow-up (B). It is easily overlooked, as bioabsorbable screws are radiolucent.
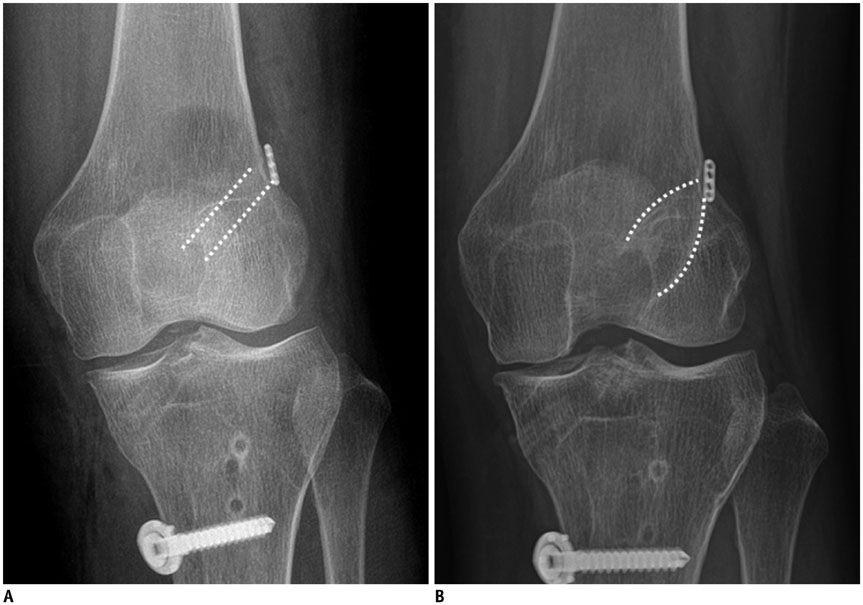
Fig. 14 Tunnel widening. Early post-operative baseline image (A), and that 2 years after surgery (B) displaying widening and loss of parallelism (> 2 mm widening) of femoral tunnel (dotted lines).
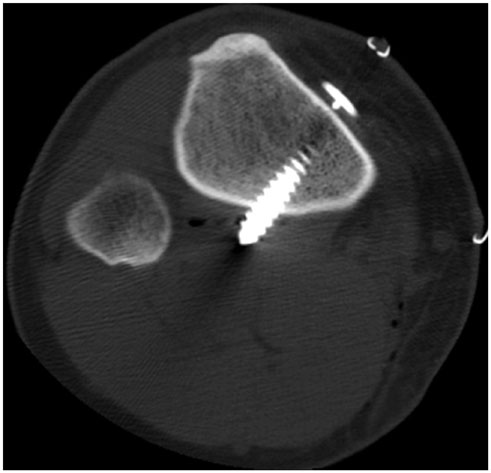
Fig. 15 Post-operative CT scan shows intramuscular location of screw tip. Patient had popliteal area pain 3 months after surgery and fixator was removed.
Cited by 1 articles
-
Value and Clinical Application of Orthopedic Metal Artifact Reduction Algorithm in CT Scans after Orthopedic Metal Implantation
Yi Hu, Shinong Pan, Xudong Zhao, Wenli Guo, Ming He, Qiyong Guo
Korean J Radiol. 2017;18(3):526-535. doi: 10.3348/kjr.2017.18.3.526.
Reference
-
1. Gianotti SM, Marshall SW, Hume PA, Bunt L. Incidence of anterior cruciate ligament injury and other knee ligament injuries: a national population-based study. J Sci Med Sport. 2009; 12:622–627.2. Janssen KW, Orchard JW, Driscoll TR, van Mechelen W. High incidence and costs for anterior cruciate ligament reconstructions performed in Australia from 2003-2004 to 2007-2008: time for an anterior cruciate ligament register by Scandinavian model? Scand J Med Sci Sports. 2012; 22:495–501.3. Adriaensen ME, Hogan B, Al-Bulushi HI, Kavanagh EC. Double-bundle depiction of the anterior cruciate ligament at 3 Tesla. Skeletal Radiol. 2012; 41:831–834.4. Casagranda BU, Maxwell NJ, Kavanagh EC, Towers JD, Shen W, Fu FH. Normal appearance and complications of double-bundle and selective-bundle anterior cruciate ligament reconstructions using optimal MRI techniques. AJR Am J Roentgenol. 2009; 192:1407–1415.5. Ng AW, Griffith JF, Hung EH, Law KY, Yung PS. MRI diagnosis of ACL bundle tears: value of oblique axial imaging. Skeletal Radiol. 2013; 42:209–217.6. Torabi M, Fu F, Luo J, Costello J. Clinical relevance and imaging features of isolated single bundle anterior cruciate tear and single bundle augmentation. Clin Imaging. 2013; 37:830–835.7. Gabriel MT, Wong EK, Woo SL, Yagi M, Debski RE. Distribution of in situ forces in the anterior cruciate ligament in response to rotatory loads. J Orthop Res. 2004; 22:85–89.8. Sakane M, Fox RJ, Woo SL, Livesay GA, Li G, Fu FH. In situ forces in the anterior cruciate ligament and its bundles in response to anterior tibial loads. J Orthop Res. 1997; 15:285–293.9. Ma Y, Deie M, Iwaki D, Asaeda M, Fujita N, Adachi N, et al. Balance ability and proprioception after single-bundle, single-bundle augmentation, and double-bundle ACL reconstruction. ScientificWorldJournal. 2014; 2014:342012.10. Bencardino JT, Beltran J, Feldman MI, Rose DJ. MR imaging of complications of anterior cruciate ligament graft reconstruction. Radiographics. 2009; 29:2115–2126.11. Tiamklang T, Sumanont S, Foocharoen T, Laopaiboon M. Double-bundle versus single-bundle reconstruction for anterior cruciate ligament rupture in adults. Cochrane Database Syst Rev. 2012; 11:CD008413.12. Trojani C, Beaufils P, Burdin G, Bussière C, Chassaing V, Djian P, et al. Revision ACL reconstruction: influence of a lateral tenodesis. Knee Surg Sports Traumatol Arthrosc. 2012; 20:1565–1570.13. Muneta T, Sekiya I, Yagishita K, Ogiuchi T, Yamamoto H, Shinomiya K. Two-bundle reconstruction of the anterior cruciate ligament using semitendinosus tendon with endobuttons: operative technique and preliminary results. Arthroscopy. 1999; 15:618–624.14. Björnsson H, Desai N, Musahl V, Alentorn-Geli E, Bhandari M, Fu F, et al. Is double-bundle anterior cruciate ligament reconstruction superior to single-bundle? A comprehensive systematic review. Knee Surg Sports Traumatol Arthrosc. 2015; 23:696–739.15. Denti M, Lo Vetere D, Bait C, Schönhuber H, Melegati G, Volpi P. Revision anterior cruciate ligament reconstruction: causes of failure, surgical technique, and clinical results. Am J Sports Med. 2008; 36:1896–1902.16. Haasper C, Kopf S, Lorenz S, Middleton KK, Tashman S, Fu FH. Influence of tibial rotation on tibial tunnel position measurements using lateral fluoroscopy in anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2015; 23:649–654.17. Lee JK, Lee S, Seong SC, Lee MC. Anatomy of the anterior cruciate ligament insertion sites: comparison of plain radiography and three-dimensional computed tomographic imaging to anatomic dissection. Knee Surg Sports Traumatol Arthrosc. 2015; 23:2297–2305.18. Bedi A, Maak T, Musahl V, O'Loughlin P, Choi D, Citak M, et al. Effect of tunnel position and graft size in single-bundle anterior cruciate ligament reconstruction: an evaluation of time-zero knee stability. Arthroscopy. 2011; 27:1543–1551.19. Bernard M, Hertel P, Hornung H, Cierpinski T. Femoral insertion of the ACL. Radiographic quadrant method. Am J Knee Surg. 1997; 10:14–21. discussion 21-22.20. Amis AA, Jakob RP. Anterior cruciate ligament graft positioning, tensioning and twisting. Knee Surg Sports Traumatol Arthrosc. 1998; 6:Suppl 1. S2–S12.21. Bird JH, Carmont MR, Dhillon M, Smith N, Brown C, Thompson P, et al. Validation of a new technique to determine midbundle femoral tunnel position in anterior cruciate ligament reconstruction using 3-dimensional computed tomography analysis. Arthroscopy. 2011; 27:1259–1267.22. Tscholl PM, Biedert RM, Gal I. Radiological evaluation for conflict of the femoral tunnel entrance area prior to anterior cruciate ligament revision surgery. Int Orthop. 2014; 38:607–615.23. Illingworth KD, Hensler D, Working ZM, Macalena JA, Tashman S, Fu FH. A simple evaluation of anterior cruciate ligament femoral tunnel position: the inclination angle and femoral tunnel angle. Am J Sports Med. 2011; 39:2611–2618.24. Parkar AP, Adriaensen ME, Strand T, Inderhaug E, Harlem T, Solheim E. How to read post-operative radiographs and CT scans after single-bundle anterior cruciate ligament reconstruction. Skeletal Radiol. 2013; 42:1489–1500.25. Howell SM, Gittins ME, Gottlieb JE, Traina SM, Zoellner TM. The relationship between the angle of the tibial tunnel in the coronal plane and loss of flexion and anterior laxity after anterior cruciate ligament reconstruction. Am J Sports Med. 2001; 29:567–574.26. Stäubli HU, Rauschning W. Tibial attachment area of the anterior cruciate ligament in the extended knee position. Anatomy and cryosections in vitro complemented by magnetic resonance arthrography in vivo. Knee Surg Sports Traumatol Arthrosc. 1994; 2:138–146.27. Howell SM, Hull ML. Checkpoints for judging tunnel and anterior cruciate ligament graft placement. J Knee Surg. 2009; 22:161–170.28. Meuffels DE, Potters JW, Koning AH, Brown CH Jr, Verhaar JA, Reijman M. Visualization of postoperative anterior cruciate ligament reconstruction bone tunnels: reliability of standard radiographs, CT scans, and 3D virtual reality images. Acta Orthop. 2011; 82:699–703.29. Yoon SJ, Yoon YC, Bae SY, Wang JH. Bone tunnel diameter measured with CT after anterior cruciate ligament reconstruction using double-bundle auto-hamstring tendons: clinical implications. Korean J Radiol. 2015; 16:1313–1318.30. Kondo E, Yasuda K, Ichiyama H, Azuma C, Tohyama H. Radiologic evaluation of femoral and tibial tunnels created with the transtibial tunnel technique for anatomic double-bundle anterior cruciate ligament reconstruction. Arthroscopy. 2007; 23:869–876.31. Yanmiş I, Tunay S, Oğuz E, Yildiz C, Ozkan H, Kirdemir V. Dropping of an EndoButton into the knee joint 2 years after anterior cruciate ligament repair using proximal fixation methods. Arthroscopy. 2004; 20:641–643.32. Mae T, Kuroda S, Matsumoto N, Yoneda M, Nakata K, Yoshikawa H, et al. Migration of EndoButton after anatomic double-bundle anterior cruciate ligament reconstruction. Arthroscopy. 2011; 27:1528–1535.33. Pereira H, Correlo VM, Silva-Correia J, Oliveira JM, Reis RL, Espregueira-Mendes J. Migration of "bioabsorbable" screws in ACL repair. How much do we know? A systematic review. Knee Surg Sports Traumatol Arthrosc. 2013; 21:986–994.34. Fauno P, Kaalund S. Tunnel widening after hamstring anterior cruciate ligament reconstruction is influenced by the type of graft fixation used: a prospective randomized study. Arthroscopy. 2005; 21:1337–1341.35. Choi NH, Lee JH, Son KM, Victoroff BN. Tibial tunnel widening after anterior cruciate ligament reconstructions with hamstring tendons using Rigidfix femoral fixation and Intrafix tibial fixation. Knee Surg Sports Traumatol Arthrosc. 2010; 18:92–97.36. Fineberg MS, Zarins B, Sherman OH. Practical considerations in anterior cruciate ligament replacement surgery. Arthroscopy. 2000; 16:715–724.37. Mithöfer K, Gill TJ, Vrahas MS. Tibial plateau fracture following anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2004; 12:325–328.38. Wang C, Ao Y, Wang J, Hu Y, Cui G, Yu J. Septic arthritis after arthroscopic anterior cruciate ligament reconstruction: a retrospective analysis of incidence, presentation, treatment, and cause. Arthroscopy. 2009; 25:243–249.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ligament Reconstruction in Congenital Absence of the Anterior Cruciate Ligament: A Case Report
- The Reconstruction of Anterior Cruciate Ligament Using Patellar Tendon under Arthroscopy
- Arthroscopic Revision Anterior Cruciate Ligament Reconstruction: Report of 5 Cases
- Anterior Cruciate Ligament Reconstruction with Achilles Tendon Allograft
- The Effect of Cyclic Tensile Load on Various Tibial Fixation Techniques in Anterior Cruciate Ligament Reconstruction
