J Bone Metab.
2019 Nov;26(4):263-270. 10.11005/jbm.2019.26.4.263.
Clinical Characteristics of Primary and Secondary Osteoporotic Fractures: Data from Single Referral Center Emergency Department
- Affiliations
-
- 1Department of Orthopaedic Surgery, Sanggye Paik Hospital, Inje University College of Medicine, Seoul, Korea. cjyortho@hanmail.net
- KMID: 2465028
- DOI: http://doi.org/10.11005/jbm.2019.26.4.263
Abstract
- BACKGROUND
To investigate the characteristics of patients with osteoporotic fractures (OF) who visited the emergency room, we analyzed the frequency and distribution of primary and secondary OF.
METHODS
From March 2015 to April 2017, 406 patients with OF were assigned to wrist (W; n=132), spine (S; n=78), and hip (H; n=196) according to the site. All subjects were classified as having primary fracture or secondary fracture. Age, fracture site, the risk of future fracture using Fracture Risk Assessment Tool (FRAX) were compared.
RESULTS
The mean age at fracture site was significantly different among the 3 groups, groups W (66.57±10.03), S (73.50±9.07), and H (78.50±7.72). The most common site of OF were in the order of wrist, spine, and hip with the increase of age. The FRAX scores significantly increased (P<0.001) in the order of W (8.35±5.67), S (10.74±6.99), and H (13.88±7.98) in total patient, and same in primary fracture group (W, 7.50±4.18; S, 9.76±5.91; H, 11.93±6.61; P<0.001). The main site of prior fractures in secondary fracture was same lesion, which means that the prior fracture of secondary wrist fracture was wrist fracture such as spine for spine, hip for hip.
CONCLUSIONS
We determined that as age increasing, the major sites of OF were different and FRAX scores increased. The most common site for secondary fracture was the same one. Hence, the risk of subsequent fracture in same site should be noted after patient suffered OF.
MeSH Terms
Figure
-

Fig. 1 Flowchart of patient inclusion and exclusion data.

Fig. 2 Distribution of the fracture sites according to age. Values are presented as the number of patients, with the percentages in parentheses.
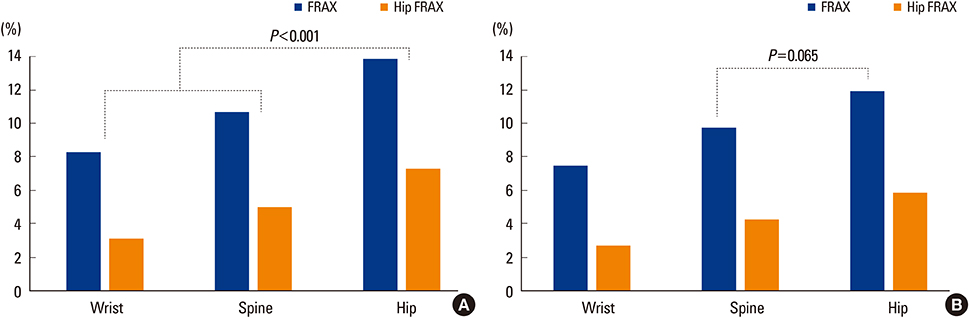
Fig. 3 Fracture Risk Assessment Tool (FRAX) & hip FRAX scores of patients. (A) Total patients. (B) Patients with first fracture episode. Bold characters indicate significant difference (P<0.05).
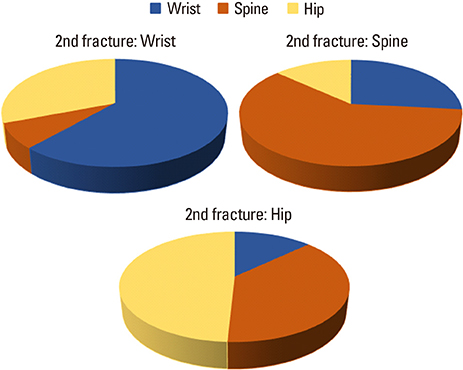
Fig. 4 Distribution of primary fracture site in different secondary fractures.
Reference
-
1. Roux C, Briot K. Imminent fracture risk. Osteoporos Int. 2017; 28:1765–1769.
Article2. Cauley JA. Osteoporosis: fracture epidemiology update 2016. Curr Opin Rheumatol. 2017; 29:150–156.
Article3. Bonafede M, Shi N, Barron R, et al. Predicting imminent risk for fracture in patients aged 50 or older with osteoporosis using US claims data. Arch Osteoporos. 2016; 11:26.
Article4. Riggs BL, Melton LJ 3rd. The worldwide problem of osteoporosis: insights afforded by epidemiology. Bone. 1995; 17:505s–511s.
Article5. Mohd-Tahir NA, Li SC. Economic burden of osteoporosis-related hip fracture in Asia: a systematic review. Osteoporos Int. 2017; 28:2035–2044.
Article6. Kim J, Lee E, Kim S, et al. Economic burden of osteoporotic fracture of the elderly in South Korea: A national survey. Value Health Reg Issues. 2016; 9:36–41.
Article7. Cobden A, Cobden SB, Camurcu Y, et al. Effects of postoperative osteoporosis treatment on subsequent fracture and the 5-year survival rates after hemiarthroplasty for hip fracture. Arch Osteoporos. 2019; 14:100.
Article8. Rossi LMM, Copes RM, Dal Osto LC, et al. Factors related with osteoporosis treatment in postmenopausal women. Medicine (Baltimore). 2018; 97:e11524.
Article9. Reynolds K, Muntner P, Cheetham TC, et al. Primary non-adherence to bisphosphonates in an integrated healthcare setting. Osteoporos Int. 2013; 24:2509–2517.
Article10. Mitchell P, Akesson K, Chandran M, et al. Implementation of models of care for secondary osteoporotic fracture prevention and orthogeriatric models of care for osteoporotic hip fracture. Best Pract Res Clin Rheumatol. 2016; 30:536–558.
Article11. Saito T, Sterbenz JM, Malay S, et al. Effectiveness of anti-osteoporotic drugs to prevent secondary fragility fractures: systematic review and meta-analysis. Osteoporos Int. 2017; 28:3289–3300.
Article12. Yoo JH, Moon SH, Ha YC, et al. Osteoporotic fracture: 2015 Position statement of the Korean society for bone and mineral research. J Bone Metab. 2015; 22:175–181.
Article13. Johansson H, Azizieh F, Al Ali N, et al. FRAX- vs. T-score-based intervention thresholds for osteoporosis. Osteoporos Int. 2017; 28:3099–3105.
Article14. McCloskey EV, Harvey NC, Johansson H, et al. FRAX updates 2016. Curr Opin Rheumatol. 2016; 28:433–441.
Article15. Kanis JA, Harvey NC, Johansson H, et al. FRAX update. J Clin Densitom. 2017; 20:360–367.
Article16. McCloskey E, Johansson H, Oden A, et al. Fracture risk assessment. Clin Biochem. 2012; 45:887–893.
Article17. Kanis JA, Johnell O, Oden A, et al. Ten year probabilities of osteoporotic fractures according to BMD and diagnostic thresholds. Osteoporos Int. 2001; 12:989–995.
Article18. Uusi-Rasi K, Karinkanta S, Tokola K, et al. Bone mass and strength and fall-related fractures in older age. J Osteoporos. 2019; 2019:5134690.
Article19. Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 2006; 17:1726–1733.
Article20. Gregg EW, Cauley JA, Seeley DG, et al. Physical activity and osteoporotic fracture risk in older women. Study of Osteoporotic Fractures Research Group. Ann Intern Med. 1998; 129:81–88.
Article21. Schousboe JT, Fink HA, Lui LY, et al. Association between prior non-spine non-hip fractures or prevalent radiographic vertebral deformities known to be at least 10 years old and incident hip fracture. J Bone Miner Res. 2006; 21:1557–1564.
Article22. Siris ES, Genant HK, Laster AJ, et al. Enhanced prediction of fracture risk combining vertebral fracture status and BMD. Osteoporos Int. 2007; 18:761–770.
Article23. Bynum JPW, Bell JE, Cantu RV, et al. Second fractures among older adults in the year following hip, shoulder, or wrist fracture. Osteoporos Int. 2016; 27:2207–2215.
Article24. Kang BJ, Lee YK, Lee KW, et al. Mortality after hip fractures in nonagenarians. J Bone Metab. 2012; 19:83–86.
Article25. Paksima N, Koval KJ, Aharanoff G, et al. Predictors of mortality after hip fracture: a 10-year prospective study. Bull NYU Hosp Jt Dis. 2008; 66:111–117.26. Villareal DT, Fontana L, Weiss EP, et al. Bone mineral density response to caloric restriction-induced weight loss or exercise-induced weight loss: a randomized controlled trial. Arch Intern Med. 2006; 166:2502–2510.
Article27. Schürer C, Wallaschofski H, Nauck M, et al. Fracture risk and risk factors for osteoporosis. Dtsch Arztebl Int. 2015; 112:365–371.
Article28. Langlois JA, Visser M, Davidovic LS, et al. Hip fracture risk in older white men is associated with change in body weight from age 50 years to old age. Arch Intern Med. 1998; 158:990–996.
Article29. Hariri AF, Almatrafi MN, Zamka AB, et al. Relationship between body mass index and T-scores of bone mineral density in the hip and spine regions among older adults with diabetes: A retrospective review. J Obes. 2019; 2019:9827403.
Article30. Bohlken J, Jacob L, Schaum P, et al. Hip fracture risk in patients with dementia in German primary care practices. Dementia (London). 2017; 16:853–864.
Article31. Downey CL, Young A, Burton EF, et al. Dementia and osteoporosis in a geriatric population: Is there a common link. World J Orthop. 2017; 8:412–423.
Article32. Kim SR, Park YG, Kang SY, et al. Undertreatment of osteoporosis following hip fractures in jeju cohort study. J Bone Metab. 2014; 21:263–268.
Article33. Miller PD, Barlas S, Brenneman SK, et al. An approach to identifying osteopenic women at increased short-term risk of fracture. Arch Intern Med. 2004; 164:1113–1120.
Article34. Wainwright SA, Marshall LM, Ensrud KE, et al. Hip fracture in women without osteoporosis. J Clin Endocrinol Metab. 2005; 90:2787–2793.
Article35. Giangregorio LM, Leslie WD, Lix LM, et al. FRAX underestimates fracture risk in patients with diabetes. J Bone Miner Res. 2012; 27:301–308.
Article36. Leib ES, Saag KG, Adachi JD, et al. Official positions for FRAX(®) clinical regarding glucocorticoids: the impact of the use of glucocorticoids on the estimate by FRAX(®) of the 10 year risk of fracture from Joint Official Positions Development Conference of the International Society for Clinical Densitometry and International Osteoporosis Foundation on FRAX(®). J Clin Densitom. 2011; 14:212–219.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Current Concepts of Vitamin D and Calcium in the Healing of Fractures
- The Epidemiology and Importance of Osteoporotic Spinal Compression Fracture in South Korea
- Vertebroplasty in the Multiple Osteoporotic Compression Fracture
- Surgical or nonsurgical treatment of osteoporotic fractures
- Conservative Treatment of Osteoporotic Spinal Fractures
