Surgical Outcomes of Cooling Composite Graft for Fingertip Amputation
- Affiliations
-
- 1Department of Plastic and Reconstructive Surgery, Hallym University Sacred Heart Hospital, Anyang, Korea.
- 2Department of Plastic and Reconstructive Surgery, Hallym University Hangang Sacred Heart Hospital, Seoul, Korea.
- 3Department of Plastic and Reconstructive Surgery, Gwangmyeong Sungae Hospital, Gwangmyeong, Korea. pshkoh@hanmail.net
- KMID: 2464469
- DOI: http://doi.org/10.12790/ahm.2019.24.4.335
Abstract
- PURPOSE
This study aimed to report the surgical outcomes of postoperative management of ice-cooling combined with moist-open dressing and intravenous prostaglandin E1 (PGE1) injection. Ice cooling as postoperative management was also discussed.
METHODS
Forty-one fingertip amputation of 38 patients between January 2007 and December 2017 were investigated retrospectively. Fingertip amputations were managed with postoperative ice bag application for 72 hours followed by moist open dressing and PGE1 injection.
RESULTS
Twenty-five composite grafts (61.0%) survived with complete healing at 8 weeks after surgery, with favorable outcomes in cases with low injury level (type I, 82.3%) and guillotine injury (77.8%). A higher survival rate was significantly correlated with female sex, guillotine injury, injury without osseous tissue (type I), and cold outdoor temperature (p<0.05). Multivariate analysis revealed that differences between types I and III injuries, injury mode, and outdoor temperature were independent clinical parameters associated with composite graft survival.
CONCLUSION
The present study reported comparable results with postoperative ice cooling in cases with low injury level, guillotine injury, and low outdoor temperature. Prospective studies on the specific parameters of ice cooling and standards of manageable postoperative care should be conducted to enhance survival.
MeSH Terms
Figure
-
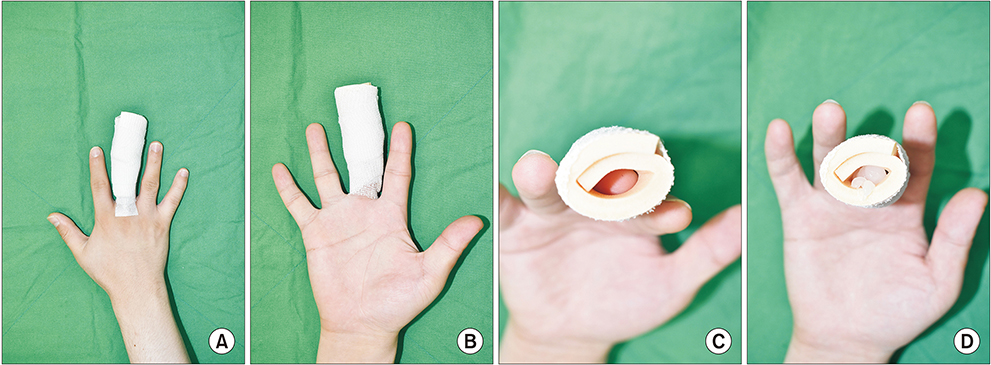
Fig. 1 Open moist dressing: (A) dorsal view, (B) palmar view, (C) fingertip view, and (D) fingertip view with ointment.

Fig. 2 Level I injury caused by crushing trauma on the right thumb of a 45-year-old male patient: (A) day of trauma day, (B) immediately postoperative, (C) postoperative day 2, and (D) postoperative day 31. The thumb showed complete survival.
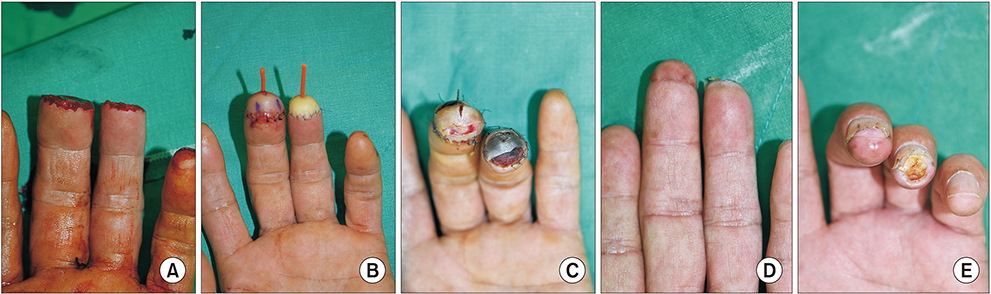
Fig. 3 Level II injury caused by guillotine injury on the left third and fourth fingers of a 56-year-old male patient: (A) day of trauma, (B) immediately postoperative, (C) postoperative day 13, (D) postoperative week 8 (anteroposterior view), and (E) postoperative week 8 (fingertip view). The third finger showed complete survival, whereas the fourth finger had partial failure.
Reference
-
1. Komatsu S, Tamai S. Successful replantation of a completely cut-off thumb. Plast Reconstr Surg. 1968; 42:374–377.
Article2. Elliot D, Moiemen NS. Composite graft replacement of digital tips. 1. Before 1850 and after 1950. J Hand Surg Br. 1997; 22:341–345.3. Hirase Y. Salvage of fingertip amputated at nail level: new surgical principles and treatments. Ann Plast Surg. 1997; 38:151–157.4. Eo S, Doh G, Lim S, Hong KY. Analysis of the risk factors that determine composite graft survival for fingertip amputation. J Hand Surg Eur Vol. 2018; 43:1030–1035.
Article5. Eo S, Hur G, Cho S, Azari KK. Successful composite graft for fingertip amputations using ice-cooling and lipo-prostaglandin E1. J Plast Reconstr Aesthet Surg. 2009; 62:764–770.
Article6. Son D, Chu H, Yeo H, Kim JH, Han K. Finger tip composite grafting managed with moist-exposed dressing. J Korean Soc Surg Hand. 2012; 17:9–15.7. Conley JJ, Vonfraenkel PH. The principle of cooling as applied to the composite graft in the nose. Plast Reconstr Surg (1946). 1956; 17:444–451.8. Das SK, Brown HG. Management of lost finger tips in children. Hand. 1978; 10:16–27.
Article9. McLaughlin CR. Composite ear grafts and their blood supply. Br J Plast Surg. 1954; 7:274–278.
Article10. Kiuchi T, Shimizu Y, Nagasao T, Ohnishi F, Minabe T, Kishi K. Composite grafting for distal digital amputation with respect to injury type and amputation level. J Plast Surg Hand Surg. 2015; 49:224–228.
Article11. Bergamini CM, Gambetti S, Dondi A, Cervellati C. Oxygen, reactive oxygen species and tissue damage. Curr Pharm Des. 2004; 10:1611–1626.
Article12. Son D, Han K, Chang DW. Extending the limits of fingertip composite grafting with moist-exposed dressing. Int Wound J. 2005; 2:315–321.
Article13. Svensjö T, Pomahac B, Yao F, Slama J, Eriksson E. Accelerated healing of full-thickness skin wounds in a wet environment. Plast Reconstr Surg. 2000; 106:602–612. discussion 613–4.
Article14. Heistein JB, Cook PA. Factors affecting composite graft survival in digital tip amputations. Ann Plast Surg. 2003; 50:299–303.
Article15. Choo J, Sparks B, Kasdan M, Wilhelmi B. Composite grafting of a distal thumb amputation: a case report and review of literature. Eplasty. 2015; 15:e5.16. Idone F, Sisti A, Tassinari J, Nisi G. Cooling composite graft for distal finger amputation: a reliable alternative to microsurgery implantation. In Vivo. 2016; 30:501–505.17. McFarlane RM, Wermuth RE. The use of hyperbaric oxygen to prevent necrosis in experimental pedicle flaps and composite skin grafts. Plast Reconstr Surg. 1966; 37:422–430.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Effect of Topical Normobaric Oxygen Therapy on Composite Graft Survival in Fingertip Amputation
- Hyperbaric Oxygen Therapy and Prostaglandin E on Composite Graft for Fingertip Amputation: Two Case Reports
- Clinical Cases of Composite Graft for Reconstruction of Fingertip Amputations using Combination Procedure of Tie-over Dressing and Drain
- Finger Tip Composite Grafting Managed with Moist-Exposed Dressing
- Effects of hyperbaric oxygen on graft survival outcomes in composite grafting for amputated fingertip injury
