Ann Rehabil Med.
2019 Oct;43(5):581-591. 10.5535/arm.2019.43.5.581.
Effectiveness of Family-Engaged Multidimensional Team Planning and Management for Recovery in Patients With Severe Stroke and Low Functional Status
- Affiliations
-
- 1Research Institute of Health and Welfare, Kibi International University, Takahashi, Japan. hiragami@kiui.ac.jp
- 2Department of Occupational Therapy, School of Rehabilitation, Hyogo University of Health Sciences, Kobe, Japan.
- KMID: 2463706
- DOI: http://doi.org/10.5535/arm.2019.43.5.581
Abstract
OBJECTIVE
To evaluate the effectiveness of family-engaged multidimensional team planning and management for patients with severe stroke and low functional status and to identify factors predictive of improved outcome at 1 month after admission.
METHODS
We retrospectively evaluated 50 patients who underwent family-engaged multidimensional rehabilitation for recovery from severe stroke due to primary unilateral cerebral lesions. The rehabilitation consisted of three phases: comprehensive multidimensional assessment, intensive rehabilitation, and evaluation. Functional Independence Measure (FIM) scores were calculated and used to predict the patients' status at discharge.
RESULTS
Although all FIM scores significantly improved after 1 month of rehabilitation, the motor FIM (mFIM) score improved the most (from 20.5±1.0 to 32.6±2.0). The total FIM (tFIM) and mFIM scores continued to improve from the first month to discharge (mean mFIM efficiency, 0.33). The high-efficiency patient group (mFIM efficiency ≥0.19) had a significantly higher discharge-to-home rate (44% vs. 13%), lower frequency of hemispatial neglect, and more severe finger numbness than the low-efficiency patient group (mFIM efficiency <0.19). The regression analyses revealed that besides lower mFIM and cognitive FIM scores at admission, unilateral spatial neglect, systemic comorbidities, and age were predictive of worse 1-month outcomes and tFIM scores (conformity, R²=0.78; predictive power, Akaike information criterion value=202).
CONCLUSION
Family-engaged multidimensional team planning and management are useful for patients with severe stroke and low functional status. Furthermore, FIM scores at admission, age, unilateral spatial neglect, and systemic comorbidities should be considered by rehabilitation teams when advising caregivers on the probability of favorable outcomes after rehabilitation.
MeSH Terms
Figure
-
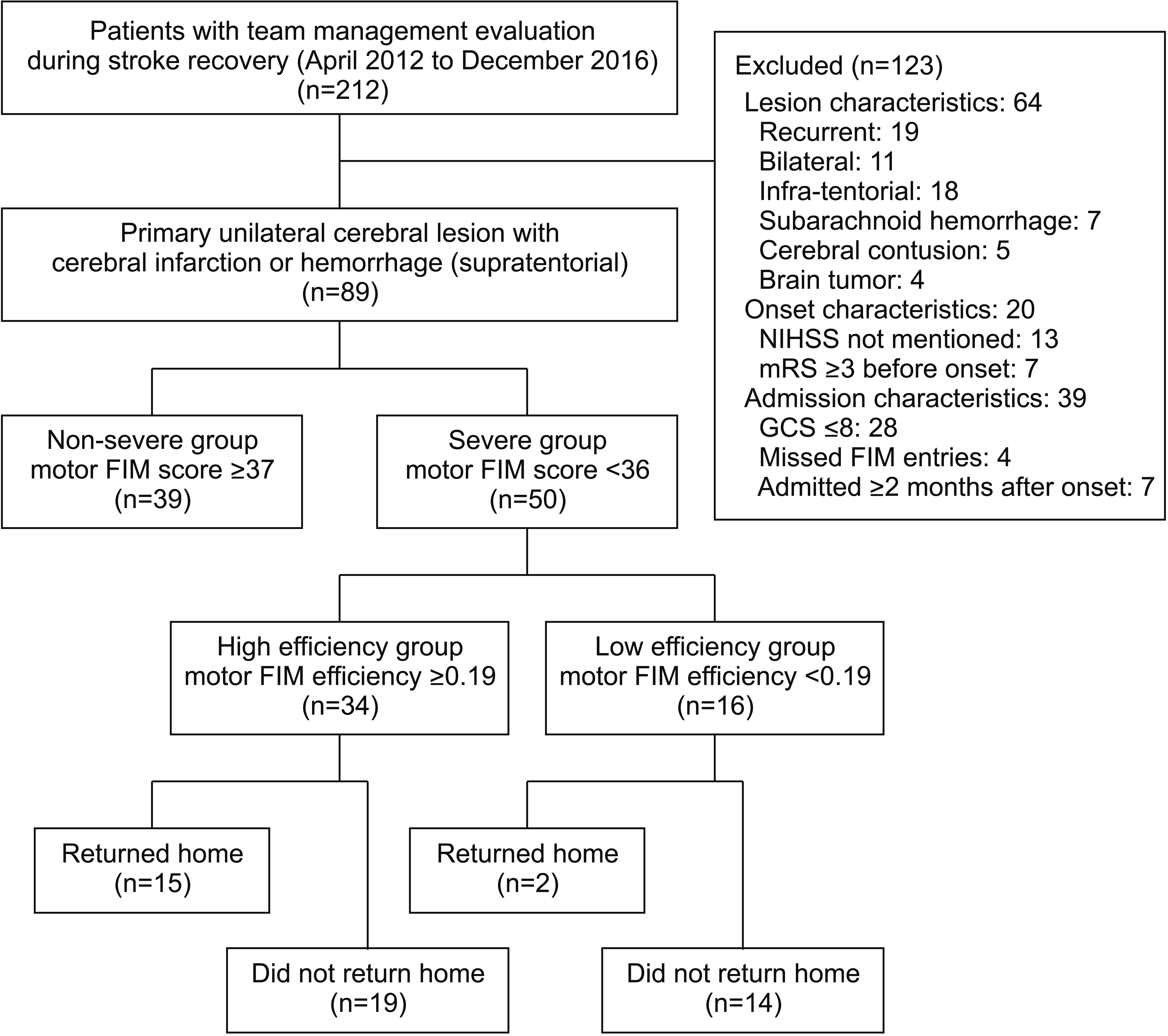
Fig. 1. Flow diagram showing the recruitment process (inclusion and exclusion criteria) and the classification of patients into study groups.
Reference
-
1. Statistics Japan. Elderly population [Internet]. Tokyo: Statistics Japan;2013. [cited 2019 Mar 21]. Available at http://www.stat.go.jp/data/topics/topi411.htm.2. Berrouschot J, Rother J, Glahn J, Kucinski T, Fiehler J, Thomalla G. Outcome and severe hemorrhagic complications of intravenous thrombolysis with tissue plasminogen activator in very old (> or =80 years) stroke patients. Stroke. 2005; 36:2421–5.3. Tsuda K, Noguchi S, Ishikawa E, Nakai Y, Akutsu H, Matsumura A. Long-term prognosis for very old patients with acute stroke. Jpn J Stroke. 2010; 32:268–74.
Article4. Mutai H, Furukawa T, Araki K, Misawa K, Hanihara T. Factors associated with functional recovery and home discharge in stroke patients admitted to a convalescent rehabilitation ward. Geriatr Gerontol Int. 2012; 12:215–22.
Article5. Toshima M, Nori K, Kanaya J, Koma K. Efficacy of rehabilitation in patients with stroke in the post-acute stage (second report: in series after admission). J Clin Rehabil. 2009; 18:659–62.6. Stineman MG, Fiedler RC, Granger CV, Maislin G. Functional task benchmarks for stroke rehabilitation. Arch Phys Med Rehabil. 1998; 79:497–504.
Article7. Kalra L, Eade J. Role of stroke rehabilitation units in managing severe disability after stroke. Stroke. 1995; 26:2031–4.
Article8. Yagura H, Miyai I, Suzuki T, Yanagihara T. Patients with severe stroke benefit most by interdisciplinary rehabilitation team approach. Cerebrovasc Dis. 2005; 20:258–63.
Article9. Kalra L, Langhorne P. Facilitating recovery: evidence for organized stroke care. J Rehabil Med. 2007; 39:97–102.
Article10. Langhorne P, Holmqvist LW; Early Supported Discharge Trialists. Early supported discharge after stroke. J Rehabil Med. 2007; 39:103–8.
Article11. Langhorne P, Pollock A; Stroke Unit Trialists’ Collaboration. What are the components of effective stroke unit care? Age Ageing. 2002; 31:365–71.
Article12. Langhorne P, Taylor G, Murray G, Dennis M, Anderson C, Bautz-Holter E, et al. Early supported discharge services for stroke patients: a meta-analysis of individual patients’ data. Lancet. 2005; 365:501–6.
Article13. Hiragami F, Nonaka T, Saitoh K, Suzuki Y. The utility of a care model to individualize rehabilitation in adults aged over 80 years. Top Stroke Rehabil. 2015; 22:102–15.
Article14. Stineman MG, Escarce JJ, Tassoni CJ, Goin JE, Granger CV, Williams SV. Diagnostic coding and medical rehabilitation length of stay: their relationship. Arch Phys Med Rehabil. 1998; 79:241–8.
Article15. Jeng JS, Huang SJ, Tang SC, Yip PK. Predictors of survival and functional outcome in acute stroke patients admitted to the stroke intensive care unit. J Neurol Sci. 2008; 270:60–6.
Article16. Hiragami F, Hiragami S, Suzuki Y. A process of multidisciplinary team communication to individualize stroke rehabilitation of an 84-year-old stroke patient. Care Manag J. 2016; 17:97–104.
Article17. Hiragami F. Introduction of a case conference using reflective methods for junior physical therapists: clinical reasoning and practical thinking process. Phys Ther Jpn. 2010; 37:127–34.18. Ministry of Health, Labour and Welfare. The 2015 general meeting of the Central Social Insurance Medical Council (Proceeding No. 316) [Internet]. Tokyo: Ministry of Health, Labour and Welfare;c2019. [cited 2019 Mar 20]. Available from: http://www.mhlw.go.jp/stf/shingi2/0000112854.html.19. Ministry of Health, Labour and Welfare. Revision of medical treatment fees for 2016 [Internet]. Tokyo: Ministry of Health, Labour and Welfare;c2019. [cited 2019 Mar 21]. Available from: http://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000106421.html.20. Gialanella B. Aphasia assessment and functional outcome prediction in patients with aphasia after stroke. J Neurol. 2011; 258:343–9.
Article21. Tokunaga M, Sannomiya K, Nakanishi R, Yonemitsu H. The external validity of multiple regression analyses predicting discharge FIM score in patients with stroke hospitalized in Kaifukuki rehabilitation wards: an analysis of the Japan Rehabilitation Database. Jpn J Compr Rehabil Sci. 2015; 6:14–20.22. Tokunaga M, Taniguchi M, Nakakado K, Mihono T, Okido A, Ushijima T, et al. Assessment of the effects of factors in stroke rehabilitation using eight multiple regression analyses: an analysis of the Japan Rehabilitation Database. Jpn J Compr Rehabil Sci. 2015; 6:78–85.23. Tokunaga M, Honda S, Miyamoto S, Torikai A, Tanaka Y, Taniwa Y, et al. Multiple regression analysis to predict each item of discharge motor FIM: analysis of Japan Rehabilitation Database. J Clin Rehabil. 2015; 24:1164–70.24. Akaike H. A new look at the statistical model identification. IEEE Trans Automat Contr. 1974; 19:716–23.
Article25. Burnham KP, Anderson DR. Multimodel inference: understanding AIC and BIC in model selection. Sociol Methods Res. 2004; 33:261–304.26. Suzuki E, Majima M, Makita S, Fuji H, Imai T. Clinical course of ischemic stroke patients measured by motor FIM in post-acute stage. Jpn J Rehabil Med. 2003; 40:302–7.
Article27. Gialanella B, Ferlucci C. Functional outcome after stroke in patients with aphasia and neglect: assessment by the motor and cognitive functional independence measure instrument. Cerebrovasc Dis. 2010; 30:440–7.
Article28. Gialanella B, Monguzzi V, Santoro R, Rocchi S. Functional recovery after hemiplegia in patients with neglect: the rehabilitative role of anosognosia. Stroke. 2005; 36:2687–90.29. Sato A, Fujita T, Konuma R, Okuda Y, Yamamoto Y, Shiomi T. Relationship between the Motor Assessment Scale at one month after admission and Functional Independent Measure at discharge in severe stroke patients. Phys Ther Jpn. 2016; 43:236–40.30. Kuwata T, Tokunaga M, Toba Y, Sannomiya K, Watanabe S, Nakanishi R, et al. The goal and objectives at the initial one month hospitalization in the stroke critical pathway in convalescent rehabilitation ward. Jpn J Phys Ther. 2008; 42:159–63.31. Katsura K, Tokunaga M, Sannomiya K, Yomemura M, Watanabe S, Hashimoto Y, et al. Mobility capacity at discharge predicted by those at entrance and at one month after entrance in patients with stroke in the convalescence rehabilitation ward. Sogo Rehabil. 2008; 36:289–95.32. Heinemann AW, Roth EJ, Cichowski K, Betts HB. Multivariate analysis of improvement and outcome following stroke rehabilitation. Arch Neurol. 1987; 44:1167–72.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Functional Recovery Status according to Rehabilitation Therapy in Stroke Patients
- Stroke Outcome and Magnetic Motor Evoked Potential
- Effect of White Matter Hyperintensity on the Functional Outcome of Ischemic Stroke Patients after Inpatient Stroke Rehabilitation
- The Influence of Depressive Symptoms on Cognitive and Functional Recovery in Chronic Stroke Patients
- Age Factor in Rehabilitation Outcome
