Minimally Invasive Surgery without Decompression for Hepatocellular Carcinoma Spinal Metastasis with Epidural Spinal Cord Compression Grade 2
- Affiliations
-
- 1Department of Neurosurgery, Spine Center, Seoul National University Bundang Hospital, Seongnam, Korea.
- 2Department of Neurosurgery, Seoul National University College of Medicine, Seoul, Korea. chungc@snu.ac.kr
- 3Department of Neurosurgery, Seoul National University Hospital, Seoul, Korea.
- 4Neuroscience Research Institute, Seoul National University Medical Research Center, Seoul, Korea.
- 5Clinical Research Institute, Seoul National University Hospital, Seoul, Korea.
- 6Department of Brain and Cognitive Sciences, Seoul National University College of Natural Sciences, Seoul, Korea.
- KMID: 2463678
- DOI: http://doi.org/10.3340/jkns.2018.0199
Abstract
OBJECTIVE
There is a lack of knowledge regarding whether decompression is necessary in treating patients with epidural spinal cord compression (ESCC) grade 2. The purpose of this study was to compare the outcomes of minimally invasive surgery (MIS) without decompression and conventional open surgery (palliative laminectomy) for patients with hepatocellular carcinoma (HCC) spinal metastasis of ESCC grade 2.
METHODS
Patients with HCC spinal metastasis requiring surgery were retrospectively reviewed. Patients with ESCC grade 2, medically intractable mechanical back pain, a Nurick grade better than 3, 3-6 months of life expectancy, Tomita score ≥5, and Spinal Instability Neoplastic Score ≥7 were included. Patients with neurological deficits, other systemic illnesses and less than 1 month of life expectancy were excluded. Thirty patients were included in the study, including 17 in the open surgery group (until 2008) and 13 in the MIS group (since 2009).
RESULTS
The MIS group had a significantly shorter operative time (94.2±48.2 minutes vs. 162.9±52.3 minutes, p=0.001), less blood loss (140.0±182.9 mL vs. 1534.4±1484.2 mL, p=0.002), and less post-operative intensive care unit transfer (one patient vs. eight patients, p=0.042) than the open surgery group. The visual analogue scale for back pain at 3 months post-operation was significantly improved in the MIS group than in the open surgery group (3.0±1.2 vs. 4.3±1.2, p=0.042). The MIS group had longer ambulation time (183±33 days vs. 166±36 days) and survival time (216±38 days vs. 204±43 days) than the open surgery group without significant difference (p=0.814 and 0.959, respectively).
CONCLUSION
MIS without decompression would be a good choice for patients with HCC spinal metastasis of ESCC grade 2, especially those with limited prognosis, mechanical instability and no neurologic deficit.
Keyword
MeSH Terms
Figure
-

Fig. 1. Epidural spinal cord compression (ESCC) grade 2. A : Schematic representation of the ESCC grade 2. A grade of 2 indicates spinal cord compression but with cerebrospinal fluid visible around the cord. B : Current neurologic, oncologic, mechanical, and systemic decision framework of grade 2 ESCC proposed by Bilsky et al [3]. cEBRT : conventional external beam radiation therapy, SRS : stereotactic radiosurgery.
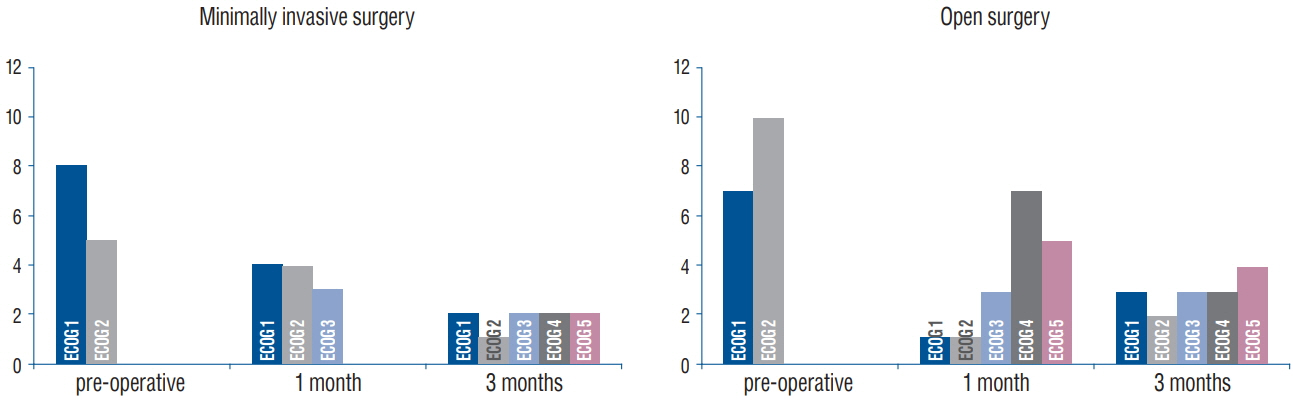
Fig. 2. Functional status (ECOG performance) changes for the minimally invasive surgery group and open surgery group pre-operatively and at postoperative 1 month and 3 months. ECOG : Eastern Cooperative Oncology Group.

Fig. 3. The mean ambulatory time for the minimally invasive surgery group was 183±33 days, and that for the open surgery group was 166± 36 days (p=0.814).
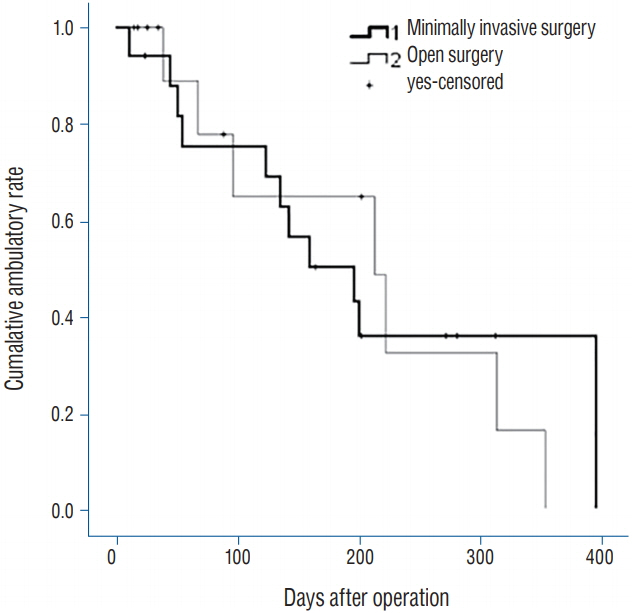
Fig. 4. The mean survival time for the minimally invasive surgery group was 216±38 days, and that for the open surgery group was 203±43 days (p=0.959).
Cited by 1 articles
-
Surgical Impacts of Metastatic Non-small Cell Lung Cancer to the Thoracic and Lumbar Spine
Jong-myung Jung, Seung-Jae Hyun, Ki-Jeong Kim
J Korean Med Sci. 2021;36(7):e52. doi: 10.3346/jkms.2021.36.e52.
Reference
-
References
1. Abrahm JL, Banffy MB, Harris MB. Spinal cord compression in patients with advanced metastatic cancer: “all I care about is walking and living my life”. JAMA. 299:937–946. 2008.
Article2. Bartels RH, van der Linden YM, van der Graaf WT. Spinal extradural metastasis: review of current treatment options. CA Cancer J Clin. 58:245–259. 2008.
Article3. Bilsky MH, Laufer I, Fourney DR, Groff M, Schmidt MH, Varga PP, et al. Reliability analysis of the epidural spinal cord compression scale. J Neurosurg Spine. 13:324–328. 2010.
Article4. Bruix J, Llovet JM. Prognostic prediction and treatment strategy in hepatocellular carcinoma. Hepatology. 35:519–524. 2002.
Article5. Chang UK, Kim MS, Han CJ, Lee DH. Clinical result of stereotactic radiosurgery for spinal metastasis from hepatocellular carcinoma: comparison with conventional radiation therapy. J Neurooncol. 119:141–148. 2014.
Article6. Cho DC, Sung JK. Palliative surgery for metastatic thoracic and lumbar tumors using posterolateral transpedicular approach with posterior instrumentation. Surg Neurol. 71:424–433. 2009.
Article7. Choi D, Crockard A, Bunger C, Harms J, Kawahara N, Mazel C, et al. Review of metastatic spine tumour classification and indications for surgery: the consensus statement of the Global Spine Tumour Study Group. Eur Spine J. 19:215–222. 2010.
Article8. Dittmer DK, Teasell R. Complications of immobilization and bed rest. Part 1: musculoskeletal and cardiovascular complications. Can Fam Physician. 39:1428–1432. 1435–1437. 1993.9. Falicov A, Fisher CG, Sparkes J, Boyd MC, Wing PC, Dvorak MF. Impact of surgical intervention on quality of life in patients with spinal metastases. Spine (Phila Pa 1976). 31:2849–2856. 2006.
Article10. Gerszten PC, Burton SA, Ozhasoglu C, Welch WC. Radiosurgery for spinal metastases: clinical experience in 500 cases from a single institution. Spine (Phila Pa 1976). 32:193–199. 2007.11. Gerszten PC, Germanwala A, Burton SA, Welch WC, Ozhasoglu C, Vogel WJ. Combination kyphoplasty and spinal radiosurgery: a new treatment paradigm for pathological fractures. J Neurosurg Spine. 3:296–301. 2005.
Article12. Gerszten PC, Monaco EA 3rd. Complete percutaneous treatment of vertebral body tumors causing spinal canal compromise using a transpedicular cavitation, cement augmentation, and radiosurgical technique. Neurosurg Focus. 27:E9. 2009.
Article13. Gerszten PC, Welch WC. Spine: minimally invasive techniques. Prog Neurol Surg. 19:135–151. 2006.
Article14. Goodwin CR, Yanamadala V, Ruiz-Valls A, Abu-Bonsrah N, Shankar G, Sankey EW, et al. A systematic review of metastatic hepatocellular carcinoma to the spine. World Neurosurg. 91:510–517.e4. 2016.
Article15. Halpin RJ, Bendok BR, Liu JC. Minimally invasive treatments for spinal metastases: vertebroplasty, kyphoplasty, and radiofrequency ablation. J Support Oncol. 2:339–351. discussion 352-355. 2004.16. Hansen-Algenstaedt N, Algenstaedt P, Böttcher A, Joscheck C, Schwarzloh B, Schaefer C, et al. Bilaterally increased VEGF-levels in muscles during experimental unilateral callus distraction. J Orthop Res. 21:805–812. 2003.
Article17. Hayat MJ, Howlader N, Reichman ME, Edwards BK. Cancer statistics, trends, and multiple primary cancer analyses from the Surveillance, Epidemiology, and End Results (SEER) program. Oncologist. 12:20–37. 2007.
Article18. Itshayek E, Yamada J, Bilsky M, Schmidt M, Shaffrey C, Gerszten P, et al. Timing of surgery and radiotherapy in the management of metastatic spine disease: a systematic review. Int J Oncol. 36:533–544. 2010.
Article19. Jansson KA, Bauer HC. Survival, complications and outcome in 282 patients operated for neurological deficit due to thoracic or lumbar spinal metastases. Eur Spine J. 15:196–202. 2006.
Article20. Jónsson B, Sjöström L, Olerud C, Andréasson I, Bring J, Rauschning W. Outcome after limited posterior surgery for thoracic and lumbar spine metastases. Eur Spine J. 5:36–44. 1996.
Article21. Kim CH, Chung CK, Jahng TA, Kim HJ. Resumption of ambulatory status after surgery for nonambulatory patients with epidural spinal metastasis. Spine J. 11:1015–1023. 2011.
Article22. Kim CH, Chung CK, Jahng TA, Kim HJ. Surgical outcome of spinal hepatocellular carcinoma metastases. Neurosurgery. 68:888–896. 2011.
Article23. Kim CH, Chung CK, Sohn S, Lee S, Park SB. Less invasive palliative surgery for spinal metastases. J Surg Oncol. 108:499–503. 2013.
Article24. Kim CW. Scientific basis of minimally invasive spine surgery: prevention of multifidus muscle injury during posterior lumbar surgery. Spine (Phila Pa 1976). 35:S281–S286. 2010.25. Kim DY, Lee SH, Chung SK, Lee HY. Comparison of multifidus muscle atrophy and trunk extension muscle strength: percutaneous versus open pedicle screw fixation. Spine (Phila Pa 1976). 30:123–129. 2005.
Article26. Kim KT, Lee SH, Suk KS, Bae SC. The quantitative analysis of tissue injury markers after mini-open lumbar fusion. Spine (Phila Pa 1976). 31:712–716. 2006.
Article27. Klimo P Jr, Kestle JR, Schmidt MH. Treatment of metastatic spinal epidural disease: a review of the literature. Neurosurg Focus. 15:E1. 2003.
Article28. Laufer I, Rubin DG, Lis E, Cox BW, Stubblefield MD, Yamada Y, et al. The NOMS framework: approach to the treatment of spinal metastatic tumors. Oncologist. 18:744–751. 2013.
Article29. Park KW, Park JW, Choi JI, Kim TH, Kim SH, Park HS, et al. Survival analysis of 904 patients with hepatocellular carcinoma in a hepatitis B virus-endemic area. J Gastroenterol Hepatol. 23:467–473. 2008.
Article30. Pascal-Moussellard H, Broc G, Pointillart V, Siméon F, Vital JM, Sénégas J. Complications of vertebral metastasis surgery. Eur Spine J. 7:438–444. 1998.
Article31. Patchell RA, Tibbs PA, Regine WF, Payne R, Saris S, Kryscio RJ, et al. Direct decompressive surgical resection in the treatment of spinal cord compression caused by metastatic cancer: a randomised trial. Lancet. 366:643–648. 2005.
Article32. Pointillart V, Vital JM, Salmi R, Diallo A, Quan GM. Survival prognostic factors and clinical outcomes in patients with spinal metastases. J Cancer Res Clin Oncol. 137:849–856. 2011.
Article33. Pull ter Gunne AF, Skolasky RL, Ross H, van Laarhoven CJ, Cohen DB. Influence of perioperative resuscitation status on postoperative spine surgery complications. Spine J. 10:129–135. 2010.
Article34. Quan GM, Vital JM, Aurouer N, Obeid I, Palussière J, Diallo A, et al. Surgery improves pain, function and quality of life in patients with spinal metastases: a prospective study on 118 patients. Eur Spine J. 20:1970–1978. 2011.
Article35. Ragel BT, Kan P, Schmidt MH. Blood transfusions after thoracoscopic anterior thoracolumbar vertebrectomy. Acta Neurochir (Wien). 152:597–603. 2010.
Article36. Schaefer C, Schroeder M, Fuhrhop I, Viezens L, Otten J, Fiedler W, et al. Primary tumor dependent inhibition of tumor growth, angiogenesis, and perfusion of secondary breast cancer in bone. J Orthop Res. 29:1251–1258. 2011.
Article37. Schneider F, Greineck F, Clausen S, Mai S, Obertacke U, Reis T, et al. Development of a novel method for intraoperative radiotherapy during kyphoplasty for spinal metastases (Kypho-IORT). Int J Radiat Oncol Biol Phys. 81:1114–1119. 2011.
Article38. Schroeder M, Viezens L, Wellbrock J, Fiedler W, Rüther W, Algenstaedt P, et al. Sunitinib treatment reduces tumor growth and limits changes in microvascular properties after minor surgical intervention in an in vivo model of secondary breast cancer growth in bone. J Surg Oncol. 113:515–521. 2016.
Article39. Schwab JH, Gasbarrini A, Cappuccio M, Boriani L, De Iure F, Colangeli S, et al. Minimally invasive posterior stabilization improved ambulation and pain scores in patients with plasmacytomas and/or metastases of the spine. Int J Surg Oncol. 2011:239230. 2011.
Article40. Sciubba DM, Gokaslan ZL. Diagnosis and management of metastatic spine disease. Surg Oncol. 15:141–151. 2006.
Article41. Sciubba DM, Petteys RJ, Dekutoski MB, Fisher CG, Fehlings MG, Ondra SL, et al. Diagnosis and management of metastatic spine disease. A review. J Neurosurg Spine. 13:94–108. 2010.42. Sohn S, Kim J, Chung CK, Lee NR, Park E, Chang UK, et al. A nationwide epidemiological study of newly diagnosed spine metastasis in the adult Korean population. Spine J. 16:937–945. 2016.
Article43. Teasell R, Dittmer DK. Complications of immobilization and bed rest. Part 2: other complications. Can Fam Physician. 39:1440–1442. 1445; -1446, 1993.44. Weigel B, Maghsudi M, Neumann C, Kretschmer R, Müller FJ, Nerlich M. Surgical management of symptomatic spinal metastases. Postoperative outcome and quality of life. Spine (Phila Pa 1976). 24:2240–2246. 1999.45. Wiesner L, Kothe R, Rüther W. Anatomic evaluation of two different techniques for the percutaneous insertion of pedicle screws in the lumbar spine. Spine (Phila Pa 1976). 24:1599–1603. 1999.
Article46. Wise JJ, Fischgrund JS, Herkowitz HN, Montgomery D, Kurz LT. Complication, survival rates, and risk factors of surgery for metastatic disease of the spine. Spine (Phila Pa 1976). 24:1943–1951. 1999.
Article47. Zairi F, Arikat A, Allaoui M, Marinho P, Assaker R. Minimally invasive decompression and stabilization for the management of thoracolumbar spine metastasis. J Neurosurg Spine. 17:19–23. 2012.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Erratum to “Minimally Invasive Surgery without Decompression for Hepatocellular Carcinoma Spinal Metastasis with Epidural Spinal Cord Compression Grade 2†by Jung JM, et al. (J Korean Neurosurg Soc 62: 467-475, 2019)
- Minimally Invasive Lateral Access Corpectomy for a Solitary Renal Cell Carcinoma Spinal Metastasis: A Case Report
- Ultra Long Construct Minimally Invasive Spinal Stabilization Using Percutaneous Pedicle Screws in the Treatment of Symptomatic Multicentric Spinal Metastasis
- Thoracic Epidural Metastasis by High Grade Neuroendocrine Carcinoma of Stomach Cancer: A Case Report
- Rapid Progression of Metastatic Clear Cell Carcinoma in Thoracic Spine: A Case Report
