Feasibility of Eye Tracking Assisted Vestibular Rehabilitation Strategy Using Immersive Virtual Reality
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Hallym University College of Medicine, Anyang, Korea. skhong96@hallym.ac.kr
- 2Laboratory of Brain and Cognitive Sciences for Convergence Medicine, Hallym University College of Medicine, Anyang, Korea.
- 3Department of Convergence Software, Hallym University, Chuncheon, Korea.
- 4Department of Otorhinolaryngology-Head and Neck Surgery, Seoul National University Bundang Hospital, Seongnam, Korea.
- KMID: 2462733
- DOI: http://doi.org/10.21053/ceo.2018.01592
Abstract
OBJECTIVES
Even though vestibular rehabilitation therapy (VRT) using head-mounted display (HMD) has been highlighted recently as a popular virtual reality platform, we should consider that HMD itself do not provide interactive environment for VRT. This study aimed to test the feasibility of interactive components using eye tracking assisted strategy through neurophysiologic evidence.
METHODS
HMD implemented with an infrared-based eye tracker was used to generate a virtual environment for VRT. Eighteen healthy subjects participated in our experiment, wherein they performed a saccadic eye exercise (SEE) under two conditions of feedback-on (F-on, visualization of eye position) and feedback-off (F-off, non-visualization of eye position). Eye position was continuously monitored in real time on those two conditions, but this information was not provided to the participants. Electroencephalogram recordings were used to estimate neural dynamics and attention during SEE, in which only valid trials (correct responses) were included in electroencephalogram analysis.
RESULTS
SEE accuracy was higher in the F-on than F-off condition (P=0.039). The power spectral density of beta band was higher in the F-on condition on the frontal (P=0.047), central (P=0.042), and occipital areas (P=0.045). Beta-event-related desynchronization was significantly more pronounced in the F-on (-0.19 on frontal and -0.22 on central clusters) than in the F-off condition (0.23 on frontal and 0.05 on central) on preparatory phase (P=0.005 for frontal and P=0.024 for central). In addition, more abundant functional connectivity was revealed under the F-on condition.
CONCLUSION
Considering substantial gain may come from goal directed attention and activation of brain-network while performing VRT, our preclinical study from SEE suggests that eye tracking algorithms may work efficiently in vestibular rehabilitation using HMD.
Figure
-
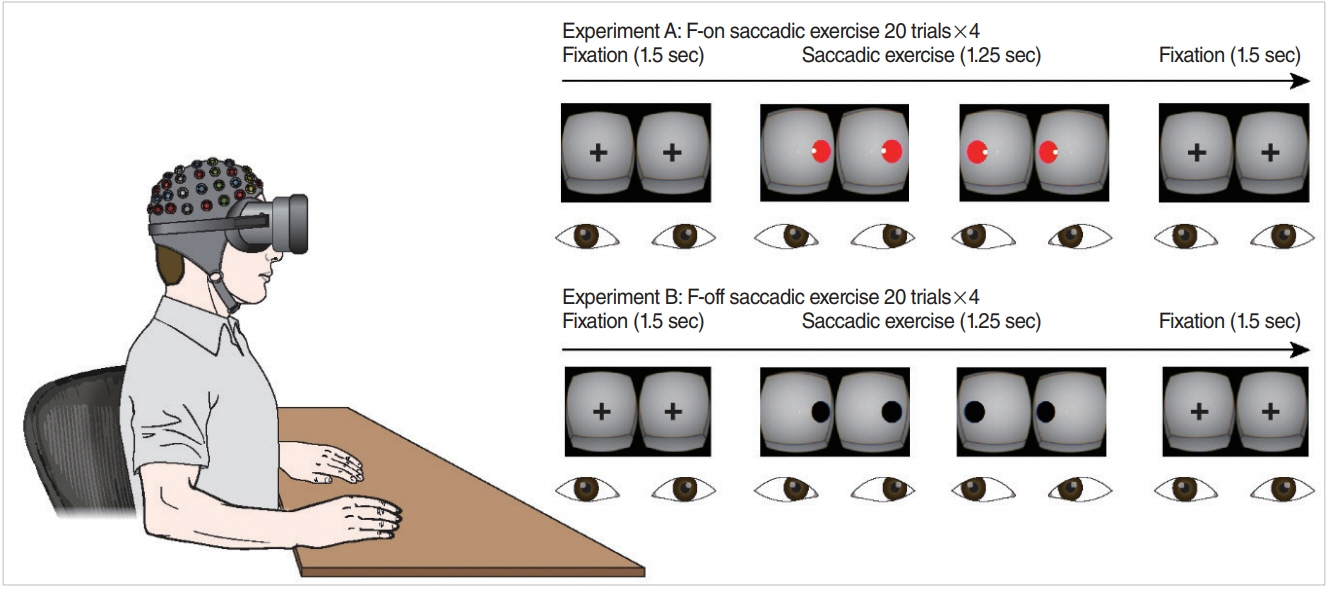
Fig. 1. Saccadic eye exercise condition under a head-mounted display and the experimental paradigm. Participants were instructed to move their eyes quickly from target to target presented at 1.25-second intervals in the virtual space and to then fix their eyes on a fixation point for 1.5 seconds. In experiment A (feedback-on [F-on] condition), participants were provided with information regarding eye position in real time (a small white circle) and feedback by changes in the visual target (from black to red) when the gaze fell on the designated visual target. Conversely, no feedback function was provided in experiment B (feedback-off [F-off] condition). Real-time eye position was continuously recorded in both conditions, but this information was not provided to the participants.
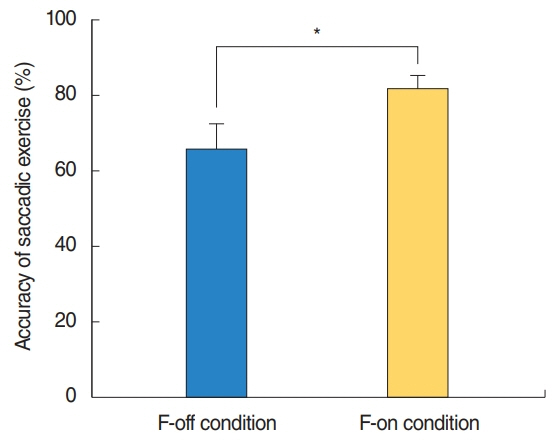
Fig. 2. Accuracy of saccadic exercise. The accuracy was 81.82%±14.13% in the feedback-on (F-on) condition and 65.71%±24.32% in the feedback-off (F-off) condition, which showed a significant difference. *P=0.039.
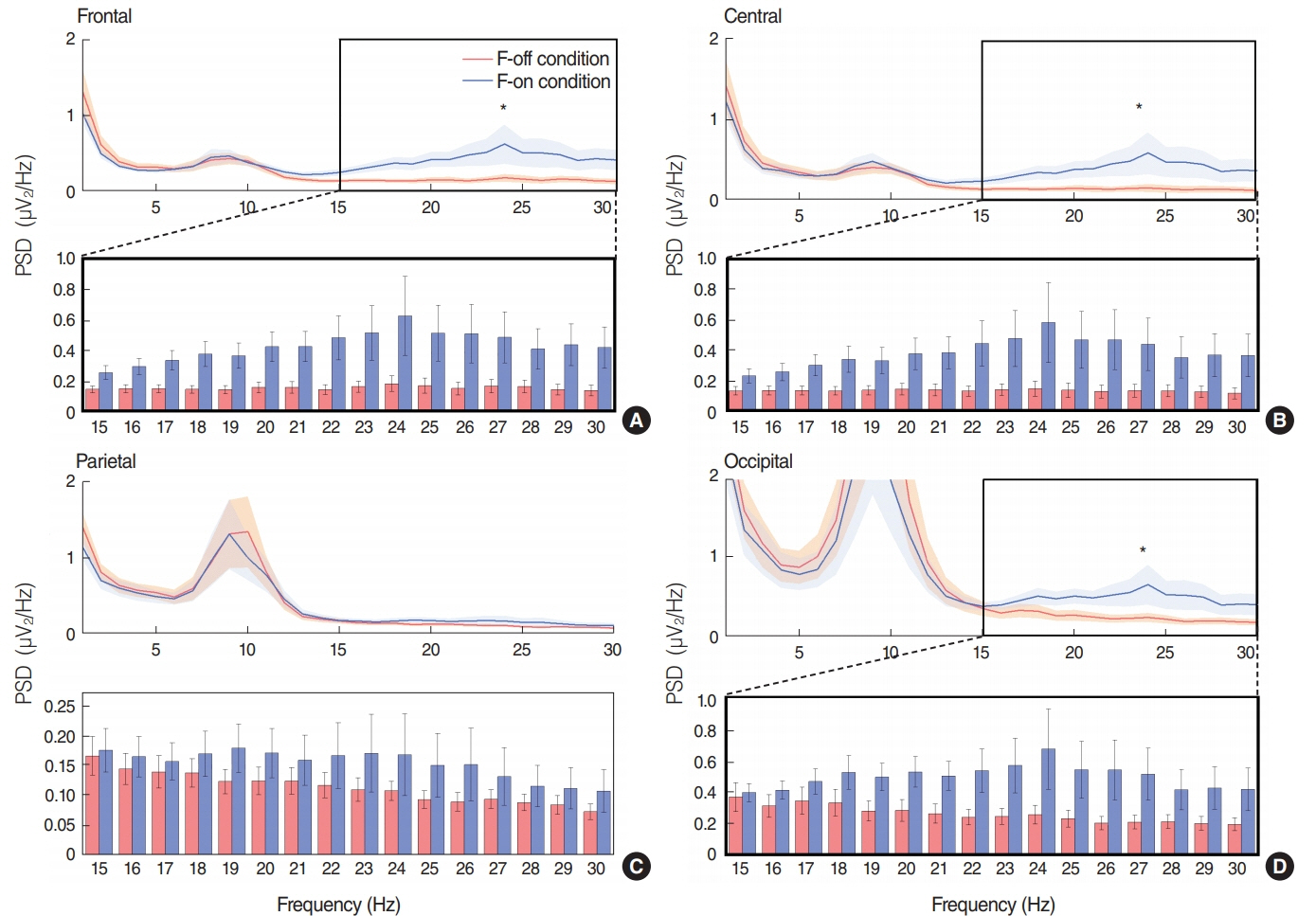
Fig. 3. Mean power spectral density (PSD) at the frontal (A), central, (B) parietal (C), and occipital (D) channel clusters. The asterisk in the thick rectangular space represents a statistically significant difference (P<0.05) between the feedback-off (F-off) and feedback-on (F-on) conditions in the given frequency bands; theta (4–7 Hz), alpha (8–12 Hz), and beta (13–30 Hz). The bottom panel in each cluster indicates a comparison of PSD between F-off versus F-on conditions in the given beta frequency range. The beta band-PSD in the frontal area, central area and occipital area were significantly higher in the F-on condition than in the F-off condition (*statistically significant differences, P=0.047 for frontal, P=0.042 for central and P=0.045 for occipital area). The error bars in each figure for PSD represent standard error of the mean from given frequency band datasets.

Fig. 4. Event-related spectral perturbation (ERSP) at the frontal (A) and central (B) channel clusters. ERSP was calculated on a prestimulation time window as −1,000 ms before the onset of target presentation (dash line) at the frontal (A) and central (B). The power level is coded on a color scale in decibels, in which synchronization appears red while desynchronization appears blue on the ERSP plots. The ERSP revealed larger beta-ERD in the feedback-on (F-on) than in the feedback-off (F-off) condition, in which mean beta-ERDs during preparatory period from –750 to –500 ms were calculated to be −0.19 on frontal and −0.22 on central area in F-on condition, whereas event-related power modulations during the same time period showed ERS (0.231 on frontal and 0.05 on central) rather than ERD pattern in F-off condition, which was statistically significant (*P=0.005 for frontal and P=0.024 for central). ERS, event-related synchronization; ERD, event-related desynchronization.
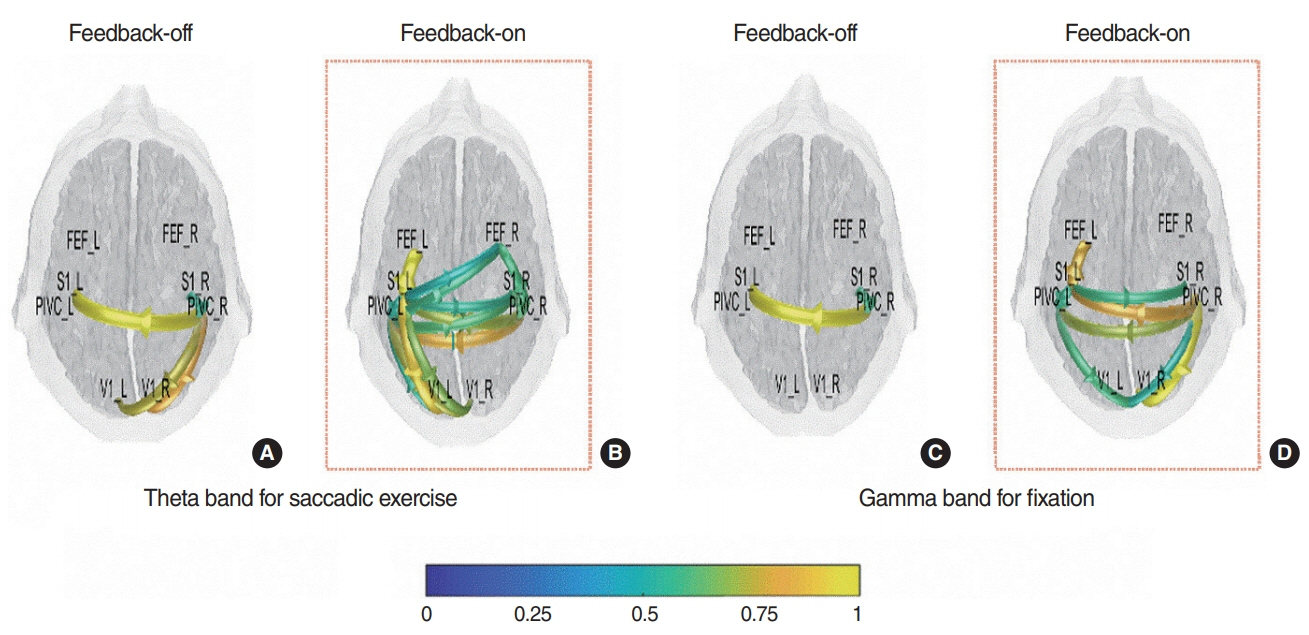
Fig. 5. Dynamic mean functional connectivity across four bilateral visual-vestibular multisensory processing-related brain regions. Functional connectivity is shown for the theta band for the saccadic period (A, B), and the gamma band for the fixation period, respectively (C, D). Scale bar represents the coefficient value using statistical assessment of surrogates (1,000 surrogate data sets, P<0.05). During the saccadic exercise period, more abundant dynamic connectivity in the theta band across the frontal eye field (FEF), primary somatosensory cortex (S1), parieto-insular vestibular cortex (PIVC) and primary visual cortex (V1) areas in the feedback-on (F-on) condition than in the feedback-off (F-off) condition was observed. In the fixation period, those from the right PIVC to the contralateral PIVC and both V1s, as well as between both S1s were observed under the F-on condition. However, no dynamic functional connectivities besides those between both PIVCs were observed under the F-off condition.
Cited by 2 articles
-
Virtual Reality for Vestibular Rehabilitation
Jae-Jun Song
Clin Exp Otorhinolaryngol. 2019;12(4):329-330. doi: 10.21053/ceo.2019.00983.Recent Advances in the Application of Artificial Intelligence in Otorhinolaryngology-Head and Neck Surgery
Bayu Adhi Tama, Do Hyun Kim, Gyuwon Kim, Soo Whan Kim, Seungchul Lee
Clin Exp Otorhinolaryngol. 2020;13(4):326-339. doi: 10.21053/ceo.2020.00654.
Reference
-
1. Cohen HS, Gottshall KR, Graziano M, Malmstrom EM, Sharpe MH. International survey of vestibular rehabilitation therapists by the Barany Society Ad Hoc Committee on Vestibular Rehabilitation Therapy. J Vestib Res. 2009; 19(1-2):15–20.
Article2. Hecker HC, Haug CO, Herndon JW. Treatment of the vertiginous patient using Cawthorne’s vestibular exercises. Laryngoscope. 1974; Nov. 84(11):2065–72.
Article3. Hillier SL, McDonnell M. Vestibular rehabilitation for unilateral peripheral vestibular dysfunction. Clin Otolaryngol. 2011; Jun. 36(3):248–9.
Article4. Bamiou DE, Luxon LM. Vertigo: clinical management and rehabilitation. In : Gleeson M, Luxon L, editors. Scott-Brown’s otorhinolaryngology, head and neck surgery. Bora Raton (FL): CRC Press;2008. p. 3791–817.5. Meldrum D, Herdman S, Vance R, Murray D, Malone K, Duffy D, et al. Effectiveness of conventional versus virtual reality-based balance exercises in vestibular rehabilitation for unilateral peripheral vestibular loss: results of a randomized controlled trial. Arch Phys Med Rehabil. 2015; Jul. 96(7):1319–28.
Article6. Pavlou M, Kanegaonkar RG, Swapp D, Bamiou DE, Slater M, Luxon LM. The effect of virtual reality on visual vertigo symptoms in patients with peripheral vestibular dysfunction: a pilot study. J Vestib Res. 2012; 22(5-6):273–81.
Article7. Alahmari KA, Sparto PJ, Marchetti GF, Redfern MS, Furman JM, Whitney SL. Comparison of virtual reality based therapy with customized vestibular physical therapy for the treatment of vestibular disorders. IEEE Trans Neural Syst Rehabil Eng. 2014; Mar. 22(2):389–99.
Article8. Yeh SC, Chen S, Wang PC, Su MC, Chang CH, Tsai PY. Interactive 3-dimensional virtual reality rehabilitation for patients with chronic imbalance and vestibular dysfunction. Technol Health Care. 2014; 22(6):915–21.
Article9. Black FO, Pesznecker SC. Vestibular adaptation and rehabilitation. Curr Opin Otolaryngol Head Neck Surg. 2003; Oct. 11(5):355–60.
Article10. Cohen HS. Disability and rehabilitation in the dizzy patient. Curr Opin Neurol. 2006; Feb. 19(1):49–54.
Article11. Bergeron M, Lortie CL, Guitton MJ. Use of virtual reality tools for vestibular disorders rehabilitation: a comprehensive analysis. Adv Med. 2015; 2015:916735.
Article12. Cooksey FS. Rehabilitation in vestibular injuries. Proc R Soc Lond B Biol Sci. 1946; Mar. 39:273–8.
Article13. Cawthorne T. The physiological basis for head exercises. J Char Soc Physiother. 1944; 3:106–7.14. Badarny S, Aharon-Peretz J, Susel Z, Habib G, Baram Y. Virtual reality feedback cues for improvement of gait in patients with Parkinson’s disease. Tremor Other Hyperkinet Mov (N Y). 2014; Apr. 4:225.15. Hong SK, Park S, Ahn MH, Min BK. Top-down and bottom-up neurodynamic evidence in patients with tinnitus. Hear Res. 2016; Dec. 342:86–100.
Article16. Makeig S, Jung TP, Bell AJ, Ghahremani D, Sejnowski TJ. Blind separation of auditory event-related brain responses into independent components. Proc Natl Acad Sci U S A. 1997; Sep. 94(20):10979–84.
Article17. Bayliss JD, Ballard DH. The effects of eye tracking in a VR helmet on EEG recordings. Rochester (NY): The University of Rochester, Computer Science Department;1998.18. Pelz JB, Hayhoe MM, Ballard DH, Shrivastava A, Bayliss JD, von der Heyde M. Development of a virtual laboratory for the study of complex human behavior. In : Merritt JO, Bolas MT, Fisher SS, editors. Stereoscopic displays and virtual reality systems VI. Bellingham: SPIE;1999.19. Delorme A, Makeig S. EEGLAB: an open source toolbox for analysis of single-trial EEG dynamics including independent component analysis. J Neurosci Methods. 2004; Mar. 134(1):9–21.
Article20. Makeig S. Auditory event-related dynamics of the EEG spectrum and effects of exposure to tones. Electroencephalogr Clin Neurophysiol. 1993; Apr. 86(4):283–93.
Article21. Yuval-Greenberg S, Tomer O, Keren AS, Nelken I, Deouell LY. Transient induced gamma-band response in EEG as a manifestation of miniature saccades. Neuron. 2008; May. 58(3):429–41.
Article22. He B, Dai Y, Astolfi L, Babiloni F, Yuan H, Yang L. eConnectome: a MATLAB toolbox for mapping and imaging of brain functional connectivity. J Neurosci Methods. 2011; Feb. 195(2):261–9.
Article23. Sohrabpour A, Ye S, Worrell GA, Zhang W, He B. Noninvasive electromagnetic source imaging and granger causality analysis: an electrophysiological connectome (eConnectome) approach. IEEE Trans Biomed Eng. 2016; Dec. 63(12):2474–87.24. Collins DL, Neelin P, Peters TM, Evans AC. Automatic 3D intersubject registration of MR volumetric data in standardized Talairach space. J Comput Assist Tomogr. 1994; Mar-Apr. 18(2):192–205.
Article25. Whitney SL, Sparto PJ, Brown KE, Furman JM, Jacobson JL, Redfern MS. The potential use of virtual reality in vestibular rehabilitation: preliminary findings with the BNAVE. J Neurol Phys Ther. 2002; 26(2):72–8.26. Gola M, Magnuski M, Szumska I, Wrobel A. EEG beta band activity is related to attention and attentional deficits in the visual performance of elderly subjects. Int J Psychophysiol. 2013; Sep. 89(3):334–41.
Article27. Kilavik BE, Zaepffel M, Brovelli A, MacKay WA, Riehle A. The ups and downs of β oscillations in sensorimotor cortex. Exp Neurol. 2013; Jul. 245:15–26.28. Kopell N, Ermentrout GB, Whittington MA, Traub RD. Gamma rhythms and beta rhythms have different synchronization properties. Proc Natl Acad Sci U S A. 2000; Feb. 97(4):1867–72.
Article29. Brinkman L, Stolk A, Dijkerman HC, de Lange FP, Toni I. Distinct roles for alpha- and beta-band oscillations during mental simulation of goal-directed actions. J Neurosci. 2014; Oct. 34(44):14783–92.
Article30. de Lange FP, Jensen O, Bauer M, Toni I. Interactions between posterior gamma and frontal alpha/beta oscillations during imagined actions. Front Hum Neurosci. 2008; Aug. 2:7.
Article31. McFarland DJ, Miner LA, Vaughan TM, Wolpaw JR. Mu and beta rhythm topographies during motor imagery and actual movements. Brain Topogr. 2000; 12(3):177–86.32. Ng TH, Sowman PF, Brock J, Johnson BW. Premovement brain activity in a bimanual load-lifting task. Exp Brain Res. 2011; Jan. 208(2):189–201.
Article33. Tzagarakis C, Ince NF, Leuthold AC, Pellizzer G. Beta-band activity during motor planning reflects response uncertainty. J Neurosci. 2010; Aug. 30(34):11270–7.
Article34. Helmchen C, Ye Z, Sprenger A, Munte TF. Changes in resting-state fMRI in vestibular neuritis. Brain Struct Funct. 2014; Nov. 219(6):1889–900.
Article35. Hong SK, Kim JH, Kim HJ, Lee HJ. Changes in the gray matter volume during compensation after vestibular neuritis: a longitudinal VBM study. Restor Neurol Neurosci. 2014; 32(5):663–73.
Article36. Dieterich M, Bauermann T, Best C, Stoeter P, Schlindwein P. Evidence for cortical visual substitution of chronic bilateral vestibular failure (an fMRI study). Brain. 2007; Aug. 130(Pt 8):2108–16.
Article37. Brandt T, Strupp M, Dieterich M. Five keys for diagnosing most vertigo, dizziness, and imbalance syndromes: an expert opinion. J Neurol. 2014; Jan. 261(1):229–31.
Article38. Schubert MC, Zee DS. Saccade and vestibular ocular motor adaptation. Restor Neurol Neurosci. 2010; 28(1):9–18.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical application of virtual reality for vestibular rehabilitation
- Correction: A Fully Immersive Virtual Reality Method for Upper Limb Rehabilitation in Spinal Cord Injury
- Motor Learning by Novel Therapeutic Approaches: Virtual Reality and Robotics
- Virtual Reality Technology Trends in Aeromedical Field
- Satisfaction and Effect Research on Virtual Reality-Based Vestibular Exercise for the Elderly Patients with Chronic Unilateral Vestibulopathy
