Influence of Patellar Tilt Angle in Merchant View on Postoperative Range of Motion in Posterior Cruciate Ligament-Substituting Fixed-Bearing Total Knee Arthroplasty
- Affiliations
-
- 1Department of Orthopaedic Surgery, Daejeon Sun Hospital, Daejeon, Korea. knee@naver.com
- KMID: 2462535
- DOI: http://doi.org/10.4055/cios.2019.11.4.416
Abstract
- BACKGROUND
We investigated whether the patellar tilt angle influences the maximum knee flexion after total knee arthroplasty (TKA) performed by using a posterior cruciate ligament-substituting (PS) fixed-bearing prosthesis in patients with relatively loose or tight flexion gap.
METHODS
In this prospective cohort study, we followed up 169 patients for at least 2 years after TKA using PS fixed-bearing prosthesis. The patients were divided into two groups according to the flexion gap value"”calculated by subtracting the thickness of the final bearing from the flexion gap measured intraoperatively under 200-cN·m force after patellar reduction and insertion of the final femoral and tibial components"”into a relatively tight group (group T; 3-6.5 mm) and a relatively loose group (group L; 7-11 mm). Patellar tilt angles and maximum non-weight-bearing active knee flexion angles were assessed postoperatively. Group T was further divided into subgroup Tn if the patellar tilt angle was < 5° and subgroup Tw if the angle was ≥ 5°. Pearson correlation test was used for the correlation analysis of the flexion gap, patellar tilt angle, and postoperative flexion range.
RESULTS
The mean postoperative flexion was 137.3° in group T and 137.5° in group L. The mean patellar tilt angle was 6.5° in group T and 6.9° in group L. In group T, a strong negative correlation (r = −0.78, p < 0.05) was observed between the patellar tilt and postoperative flexion range. However, further analysis revealed that only the subgroup Tw showed a strong negative correlation (r = −0.76, p < 0.05). Significant correlations were not found in the subgroup Tn and group L.
CONCLUSIONS
In TKA where a relatively tight flexion gap (≤ 6.5 mm) is created because of concerns about postoperative flexion instability due to a loose flexion gap, the patellar tilt angle should be < 5° for maximal postoperative knee flexion.
Keyword
MeSH Terms
Figure
-
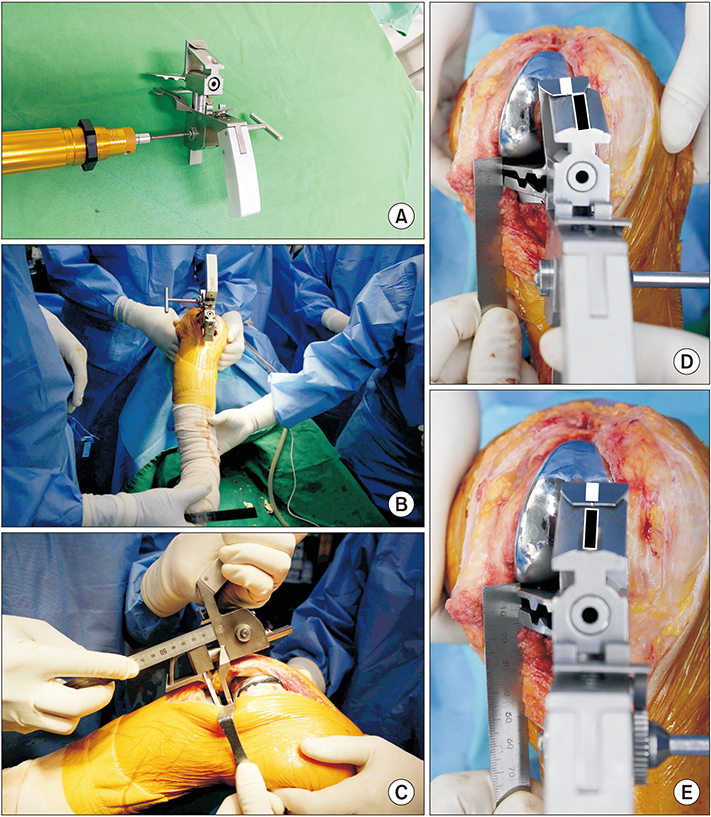
Fig. 1 Flexion gap measurement method. (A) The flexion gap was measured under 200 cN·m force exerted by a tensor device and a torque driver. (B, C) The scale at the center of the tensor device balancer shows the balance between the medial and lateral gaps. We assembled a torque driver to the rack of the balancer and measured the gap distance across the two plates. (D) If the lateral gap is wider than the medial gap (unbalanced trapezoidal flexion gap), the white bar is not in parallel to the black bar due to the scissor effect on the tensor device. (E) However, when medial and lateral flexion gaps become equal after medial collateral ligament release, the white line is parallel to the black line on the tensor device in balanced quadrangular flexion gap.

Fig. 2 Patellar tilt was measured as the angle between a line connecting the medial and lateral corners of the patella and another line connecting the anterior apex of medial and lateral femoral component condyles.
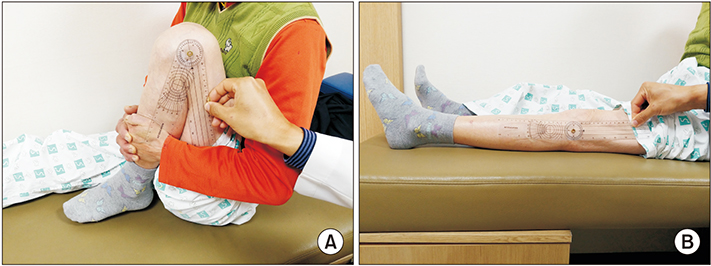
Fig. 3 Measurement of self-passive flexion (A) and extension (B) angles of the knee. Using a goniometer, we measured the intersection angle between midlines in the thigh and leg.

Fig. 4 Correlation between postoperative flexion and patellar tilt in Pearson correlation test in group T: a strong negative correlation (r = −0.78, p < 0.05) was observed. Group T: the group with a relatively tight flexion gap (3–6.5 mm).
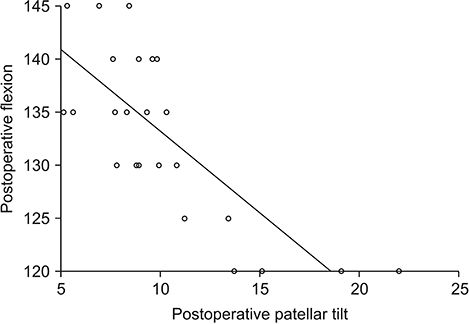
Fig. 5 Correlation between postoperative flexion and patellar tilt in Pearson correlation test in subgroup Tw. Of group T, the subgroup Tw with a patellar tilt ≥ 5° showed a strong negative correlation (r = −0.76, p < 0.05)
Reference
-
1. Callahan CM, Drake BG, Heck DA, Dittus RS. Patient outcomes following tricompartmental total knee replacement: a meta-analysis. JAMA. 1994; 271(17):1349–1357.
Article2. Dieppe P, Basler HD, Chard J, et al. Knee replacement surgery for osteoarthritis: effectiveness, practice variations, indications and possible determinants of utilization. Rheumatology (Oxford). 1999; 38(1):73–83.
Article3. Li PH, Wong YC, Wai YL. Knee flexion after total knee arthroplasty. J Orthop Surg (Hong Kong). 2007; 15(2):149–153.
Article4. Rorabeck CH, Murray P. The cost benefit of total knee arthroplasty. Orthopedics. 1996; 19(9):777–779.
Article5. Anouchi YS, McShane M, Kelly F Jr, Elting J, Stiehl J. Range of motion in total knee replacement. Clin Orthop Relat Res. 1996; (331):87–92.
Article6. Dennis DA, Komistek RD, Stiehl JB, Walker SA, Dennis KN. Range of motion after total knee arthroplasty: the effect of implant design and weight-bearing conditions. J Arthroplasty. 1998; 13(7):748–752.
Article7. Maloney WJ, Schurman DJ. The effects of implant design on range of motion after total knee arthroplasty: total condylar versus posterior stabilized total condylar designs. Clin Orthop Relat Res. 1992; (278):147–152.8. Parsley BS, Engh GA, Dwyer KA. Preoperative flexion: does it influence postoperative flexion after posterior-cruciateretaining total knee arthroplasty? Clin Orthop Relat Res. 1992; (275):204–210.9. Cho SH, Ha YC, Song HR, et al. High flex knee arthroplasty and range of motion. J Korean Orthop Assoc. 2004; 39(6):662–667.
Article10. Cho WS, Park JH, Kim JM, Hwang WY, Nam TS. Factors affecting range of motion after total knee arthroplasty. J Korean Orthop Assoc. 2003; 38(7):683–688.
Article11. Jung WH, Ha YC, Lee JS. Range of motion after high-flexion posterior stabilized total knee arthroplasty: minimum 3-year follow up. J Korean Orthop Assoc. 2007; 42(1):64–70.
Article12. Yamazaki J, Ishigami S, Nagashima M, Yoshino S. Hy-Flex II total knee system and range of motion. Arch Orthop Trauma Surg. 2002; 122(3):156–160.
Article13. Higuchi H, Hatayama K, Shimizu M, Kobayashi A, Kobayashi T, Takagishi K. Relationship between joint gap difference and range of motion in total knee arthroplasty: a prospective randomised study between different platforms. Int Orthop. 2009; 33(4):997–1000.
Article14. Bengs BC, Scott RD. The effect of patellar thickness on intraoperative knee flexion and patellar tracking in total knee arthroplasty. J Arthroplasty. 2006; 21(5):650–655.
Article15. Fukagawa S, Matsuda S, Mizu-uchi H, Miura H, Okazaki K, Iwamoto Y. Changes in patellar alignment after total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2011; 19(1):99–104.
Article16. Kawamura H, Bourne RB. Factors affecting range of flexion after total knee arthroplasty. J Orthop Sci. 2001; 6(3):248–252.
Article17. Kotani A, Yonekura A, Bourne RB. Factors influencing range of motion after contemporary total knee arthroplasty. J Arthroplasty. 2005; 20(7):850–856.
Article18. Kim JH, Yoo BW, Kim CW. Influence of the rotational alignment of the femoral and patellar components on patellar tilt in total knee arthroplasty. Knee Surg Relat Res. 2015; 27(3):163–167.
Article19. Kainz H, Reng W, Augat P, Wurm S. Influence of total knee arthroplasty on patellar kinematics and contact characteristics. Int Orthop. 2012; 36(1):73–78.
Article20. Dhollander AA, Bassens D, Victor J, Verdonk P. Patellar tilt and thickness do not influence postoperative flexion in a high-flex design total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2013; 21(12):2817–2822.21. Miyagi T, Matsuda S, Miura H, et al. Changes in patellar tracking after total knee arthroplasty: 10-year follow-up of Miller-Galante I knees. Orthopedics. 2002; 25(8):811–813.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Dislocation of Tibial Insert after Fixed Bearing TKA using Minimal Invasive Surgery: A Case Report
- Analysis of Impingement between Patella Bone and Bearing Post in Cruciate-Substituting High-Flexion Total Knee Arthroplasty
- Total Knee Arthroplasty with PCL Substituting Medial Pivot Knee: Short-term Follow-up Results
- Discrepancies of Patellofemoral Indices between Supine and Standing Merchant Views
- Results of Posterior Cruciate Retaining and Cruciate Substituting Total Knee Arthroplasty (3 to 8 years follow up)
