Clin Orthop Surg.
2019 Dec;11(4):380-387. 10.4055/cios.2019.11.4.380.
Metabolic and Hemodynamic Results and Early Complications in Simultaneous Bilateral versus Unilateral Hip Arthroscopy
- Affiliations
-
- 1Orthopedics and Traumatology-Hip Preservation Unit, Institute of Osteoarticular Diseases, Centro Médico Imbanaco, Cali, Colombia. baguilera@imbanaco.com.co
- 2Department of Anesthesiology, Centro Médico Imbanaco, Cali, Colombia.
- 3Hip Preservation Unit, Institute of Osteoarticular Diseases, Centro Médico Imbanaco, Pontificia Universidad Javeriana de Cali, Cali, Colombia.
- 4Research Institute, Centro Médico Imbanaco, Cali, Colombia.
- KMID: 2462530
- DOI: http://doi.org/10.4055/cios.2019.11.4.380
Abstract
- BACKGROUND
To compare the hemodynamic parameters"”electrolyte concentration, D-dimer level, creatine phosphokinase level"”and the incidence of early complications of simultaneous bilateral versus unilateral hip arthroscopy.
METHODS
A prospective study was conducted on patients (> 18 years of age) undergoing unilateral or bilateral hip arthroscopy under the same anesthetic between 2013 and 2015. Patients were followed up for 30 days after surgery. In all cases, data were collected before, during, and after the surgical procedure.
RESULTS
One hundred cases of hip arthroscopy (51 unilateral and 49 bilateral) were included in this study. There was a greater variation in systolic blood pressure and heart rate in the unilateral group. The sodium levels were higher in the bilateral group with an adjusted mean difference of 5.31 mmol/L (p < 0.001). During the first 24 hours after the procedure, the proportion of patients with an altered D-dimer of > 500 ng/mL was 85.7% in the bilateral group and 56.9% in the unilateral group. There was no significant difference in the incidence of complications between the groups (bilateral, 8.2%; unilateral, 9.8%; crude odds ratio, 0.83; 95% confidence interval, 0.24 to 2.92; p = 0.526).
CONCLUSIONS
The variations of hemodynamic parameters in patients undergoing hip arthroscopy remained within normal ranges. The findings of this study suggest that bilateral hip arthroscopy be selected according to the patient's condition, considering that the risk of complications and metabolic alterations in bilateral hip arthroplasty are similar to those in unilateral arthroscopy.
Keyword
MeSH Terms
Figure
-
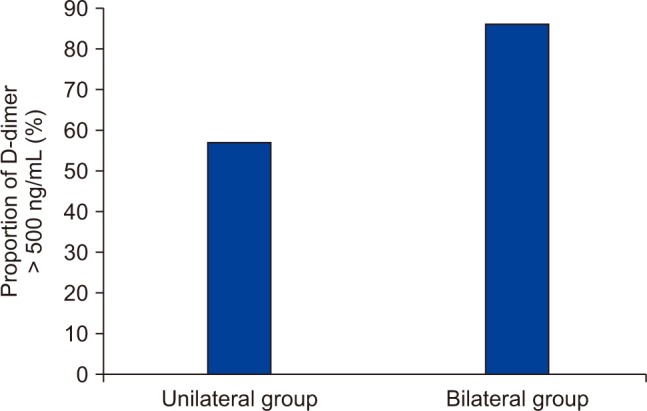
Fig. 1 Percent of D-dimer level > 500 ng/mL after unilateral and bilateral arthroscopy.
Reference
-
1. Glick JM, Valone F 3rd, Safran MR. Hip arthroscopy: from the beginning to the future: an innovator's perspective. Knee Surg Sports Traumatol Arthrosc. 2014; 22(4):714–721. PMID: 24482213.2. Clarke MT, Arora A, Villar RN. Hip arthroscopy: complications in 1054 cases. Clin Orthop Relat Res. 2003; (406):84–88.
Article3. Truntzer JN, Hoppe DJ, Shapiro LM, Abrams GD, Safran M. Complication rates for hip arthroscopy are underestimated: a population-based study. Arthroscopy. 2017; 33(6):1194–1201. PMID: 28259588.
Article4. Pollard TC, Villar RN, Norton MR, et al. Genetic influences in the aetiology of femoroacetabular impingement: a sibling study. J Bone Joint Surg Br. 2010; 92(2):209–216. PMID: 20130310.5. Kang AC, Gooding AJ, Coates MH, Goh TD, Armour P, Rietveld J. Computed tomography assessment of hip joints in asymptomatic individuals in relation to femoroacetabular impingement. Am J Sports Med. 2010; 38(6):1160–1165. PMID: 20228244.
Article6. Allen D, Beaule PE, Ramadan O, Doucette S. Prevalence of associated deformities and hip pain in patients with camtype femoroacetabular impingement. J Bone Joint Surg Br. 2009; 91(5):589–594. PMID: 19407290.
Article7. Beck M, Kalhor M, Leunig M, Ganz R. Hip morphology influences the pattern of damage to the acetabular cartilage: femoroacetabular impingement as a cause of early osteoarthritis of the hip. J Bone Joint Surg Br. 2005; 87(7):1012–1018. PMID: 15972923.8. Haviv B, O'Donnell J. Arthroscopic treatment for symptomatic bilateral cam-type femoroacetabular impingement. Orthopedics. 2010; 33(12):874. PMID: 21162505.
Article9. Degen RM, Nawabi DH, Fields KG, Wentzel CS, Kelly BT, Coleman SH. Simultaneous versus staged bilateral hip arthroscopy in the treatment of femoroacetabular impingement. Arthroscopy. 2016; 32(7):1300–1307. PMID: 27129376.
Article10. Mather RC, Reddy A, Nho SJ. Complications of hip arthroscopy. In : Byrd JW, editor. Operative hip arthroscopy. Operative hip arthroscopy: Springer-Verlag New York;2012. p. 403–409.11. Martin HD, Palmer IJ, Champlin K, Kaiser B, Kelly B, Leunig M. Physiological changes as a result of hip arthroscopy performed with traction. Arthroscopy. 2012; 28(10):1365–1372. PMID: 22920287.
Article12. Hargett CW, Tapson VF. Clinical probability and D-dimer testing: how should we use them in clinical practice? Semin Respir Crit Care Med. 2008; 29(1):15–24. PMID: 18302083.
Article13. Adam SS, Key NS, Greenberg CS. D-dimer antigen: current concepts and future prospects. Blood. 2009; 113(13):2878–2887. PMID: 19008457.
Article14. Morandi L, Angelini C, Prelle A, et al. High plasma creatine kinase: review of the literature and proposal for a diagnostic algorithm. Neurol Sci. 2006; 27(5):303–311. PMID: 17122938.
Article15. Molina CS, Thakore RV, Blumer A, Obremskey WT, Sethi MK. Use of the national surgical quality improvement program in orthopaedic surgery. Clin Orthop Relat Res. 2015; 473(5):1574–1581. PMID: 24706043.
Article16. Verhelst L, De Schepper J, Sergeant G, Liekens K, Delport H. Variations in serum electrolyte concentrations and renal function after therapeutic hip arthroscopy: a pilot study. Arthroscopy. 2009; 25(4):377–381. PMID: 19341924.
Article17. Piper GL, Kaplan LJ. Fluid and electrolyte management for the surgical patient. Surg Clin North Am. 2012; 92(2):189–205. PMID: 22414407.
Article18. Hug CC Jr, McLeskey CH, Nahrwold ML, et al. Hemodynamic effects of propofol: data from over 25,000 patients. Anesth Analg. 1993; 77(4 Suppl):S21–S29. PMID: 8214693.19. Parodi D, Valderrama J, Tobar C, et al. Effect of warmed irrigation solution on core body temperature during hip arthroscopy for femoroacetabular impingement. Arthroscopy. 2014; 30(1):36–41. PMID: 24183196.
Article20. Nakano N, Khanduja V. Complications in hip arthroscopy. Muscles Ligaments Tendons J. 2016; 6(3):402–409. PMID: 28066747.
Article21. Parodi D, Tobar C, Valderrama J, et al. Hip arthroscopy and hypothermia. Arthroscopy. 2012; 28(7):924–928. PMID: 22386065.
Article22. Dindo D, Breitenstein S, Hahnloser D, et al. Kinetics of D-dimer after general surgery. Blood Coagul Fibrinolysis. 2009; 20(5):347–352. PMID: 19474701.
Article23. Sudo A, Wada H, Nobori T, et al. Cut-off values of D-dimer and soluble fibrin for prediction of deep vein thrombosis after orthopaedic surgery. Int J Hematol. 2009; 89(5):572–576. PMID: 19430861.
Article24. Harris JD, McCormick FM, Abrams GD, et al. Complications and reoperations during and after hip arthroscopy: a systematic review of 92 studies and more than 6,000 patients. Arthroscopy. 2013; 29(3):589–595. PMID: 23544691.
Article25. Park MS, Yoon SJ, Kim YJ, Chung WC. Hip arthroscopy for femoroacetabular impingement: the changing nature and severity of associated complications over time. Arthroscopy. 2014; 30(8):957–963. PMID: 24835839.
Article26. Clohisy JC, Baca G, Beaule PE, et al. Descriptive epidemiology of femoroacetabular impingement: a North American cohort of patients undergoing surgery. Am J Sports Med. 2013; 41(6):1348–1356. PMID: 23669751.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comprehensive Review of Advancements in Hip Arthroscopy
- Arthroscopy of the Hip Joint: Diagnosis and Treatment
- Bilateral Asymmetric Traumatic Dislocation of the Hip Joint
- Bilateral Simultaneous Bell's Palsy-Two Case Studies
- Traumatic Simultaneous Bilateral Hip Dislocation in the Elderly Patient: A Case Report
