A case of unexpected adjacent tooth extrusion after implant fixed prosthetic treatment, who had undergone mandibular resection and reconstruction due to ameloblastoma
- Affiliations
-
- 1Department of Prosthodontics, School of Dentistry, Yonsei University, Seoul, Republic of Korea. jee917@yuhs.ac
- 2Department of Oral and Maxillofacial Surgery, School of Dentistry, Yonsei University, Seoul, Republic of Korea.
- KMID: 2461153
- DOI: http://doi.org/10.4047/jkap.2019.57.4.448
Abstract
- Ameloblastoma is a benign odontogenic epithelial tumor with high recurrence rate and requires extensive resection of the surrounding tissue and reconstruction of defect site. Because of the anatomical limitation of the reconstruction site, prosthetic treatment with implants is the first recommendation. This is a case of prosthetic restoration of the reconstruction site with implant fixed prosthesis in patient who underwent mandibular resection and iliac bone reconstruction due to ameloblastoma. However 14 months after completion of implant prosthesis, adjacent natural tooth erupted unexpectedly, resulting in 1mm infra-occlusion occurred including posterior implant prosthesis and anterior natural teeth. In adults, implant infra-occlusion may occur due to residual growth after placement of the maxillary anterior implant. But this case, hypo-occlusion of molar implant and open bite of anterior natural teeth is occurred due to extrusion of adjacent tooth, is rare. Thus we report the treatment process including orthodontic treatment with intrusion of the posterior tooth, and investigate the causes of sudden, unexpected tooth extrusion.
MeSH Terms
Figure
-
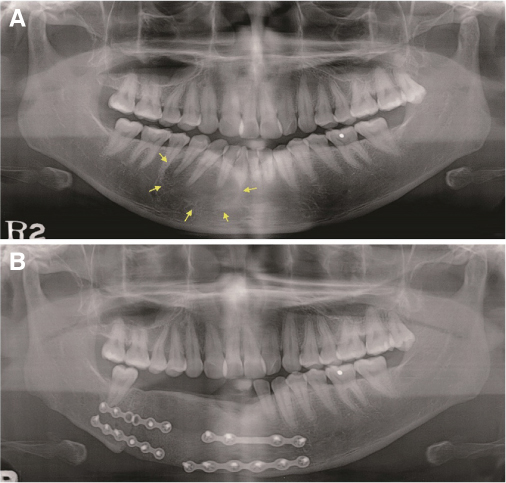
Fig. 1 Panoramic radiographic examination. (A) Pre-operative radiographic examination. Arrows indicate the boundaries of ameloblastoma, (B) After segmental mandibulectomy and reconstruction of right mandible with iliac bone graft.

Fig. 2 (A) Post opeative intraoral examination, (B) With a temporary denture.
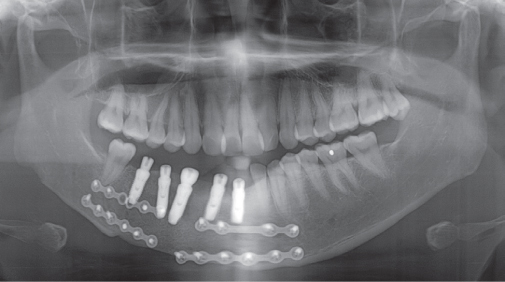
Fig. 3 Radiographic examination after placement of implants in mandibular reconstruction area.

Fig. 4 (A) Temporary implant fixed prosthesis made of polymethyl methacrylate, (B) Final implant prosthesis made of zirconia. The shape and occlusion of prosthesis verified with temporary restorations were reflected.

Fig. 5 (A) Two-months checkup after delivery. No pathologic changes were found except the exposed fixture (second molar), (B) Fourteen-months checkup after delivery. Except the second molar, any implant prosthesis was not occluded with shimstock inspection, (C) Two-years checkup after delivery. Occlusal change progressed further, the implant prosthesis except for the second molar showed an open bite to the naked eye. Compared with two-months checkup radiograph, (A), the last posterior nature tooth was extruded.
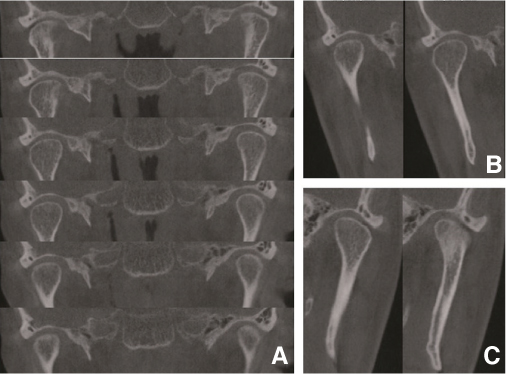
Fig. 6 Computed tomography images for temporomandibular joint. There are no signs of osteoarthritis. (A) Coronal view, (B) Axial view of right temporomandibular complex, (C) Axial view of left temporomandibular complex.
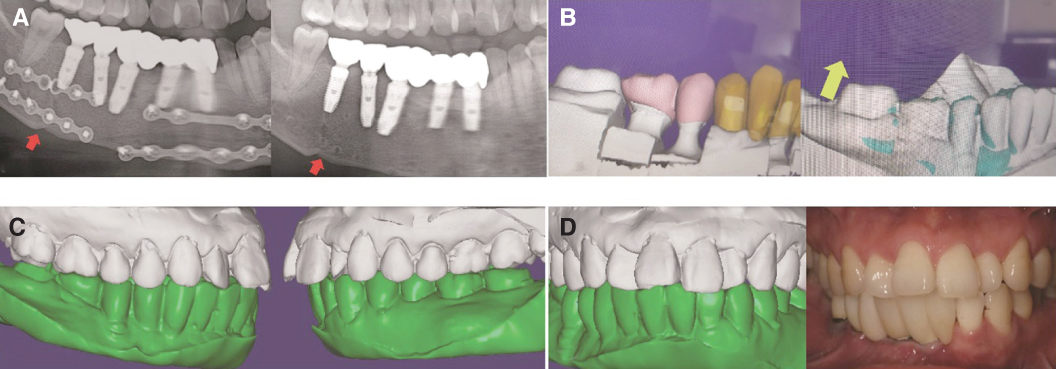
Fig. 7 Analysis to determine whether or not the posterior tooth was extruded. (A) Radiographically, there is no sign of sinking of the graft bone segment. Arrows indicate the joint between graft bone segment and mandible, (B) Comparison of dental models. Left image is the model used to design the implant prosthesis, right image is the model after open bite. Clinical crown length of the second molar became longer, (C) In order to confirm the occlusal change of the remaining teeth except the last molar, the occlusal surface of the second molar of study model was removed and the casts were occluded, (D) When the extruded surface of the second molar of study model was removed, the maxillary and mandibular models were engaged with previous occlusion.

Fig. 8 Intraoral examination. (A) At the time of open bite, (B) During orthodontic treatment. Open bite is alleviating when the last posterior mouth is intruded.
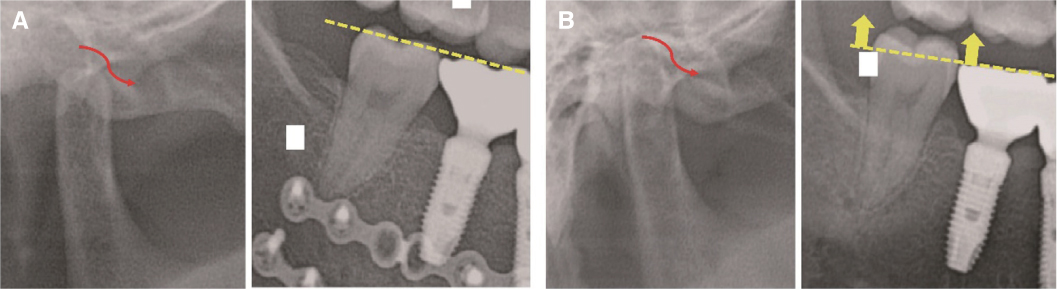
Fig. 9 Hypothesis about extrusion of the posterior tooth due to condylar sag. (A) Condyle to move medially and slide inferiorly on the medial wall of the fossa causing a posterior open bite, (B) The most posterior tooth which lost occlusion was extruded.
Reference
-
1. Brad WN, Douglas DD, Carl ML, Jerry EB. Oral and maxillofacial pathology. 2nd ed. Philadelphia: Elsevier Saunders;2002. p. 611–619.2. Wong HH, Pow EH, Choi WW. Management of mandibular rotation after a mandibulectomy: a clinical report. J Prosthet Dent. 2013; 110:532–537.
Article3. Garrett N, Roumanas ED, Blackwell KE, Freymiller E, Abemayor E, Wong WK, Gerratt B, Berke G, Beumer J 3rd, Kapur KK. Efficacy of conventional and implant-supported mandibular resection prostheses: study overview and treatment outcomes. J Prosthet Dent. 2006; 96:13–24.
Article4. Chiapasco M, Colletti G, Romeo E, Zaniboni M, Brusati R. Long-term results of mandibular reconstruction with autogenous bone grafts and oral implants after tumor resection. Clin Oral Implants Res. 2008; 19:1074–1080.
Article5. Cheung LK, Leung AC. Dental implants in reconstructed jaws: implant longevity and peri-implant tissue outcomes. J Oral Maxillofac Surg. 2003; 61:1263–1274.
Article6. Zitzmann NU, Arnold D, Ball J, Brusco D, Triaca A, Verna C. Treatment strategies for infraoccluded dental implants. J Prosthet Dent. 2015; 113:169–174.
Article7. Oesterle LJ, Cronin RJ Jr. Adult growth, aging, and the singletooth implant. Int J Oral Maxillofac Implants. 2000; 15:252–260.8. Korean Academy of Orofacial Pain and Oral Medicine. Orofacial pains and temporomandibular disorders. 4th ed. Seoul: Yenang;2012. p. 146–161.9. Reyneke JP, Ferretti C. Intraoperative diagnosis of condylar sag after bilateral sagittal split ramus osteotomy. Br J Oral Maxillofac Surg. 2002; 40:285–292.
Article10. Hiatt WR, Schelkun PM, Moore DL. Condylar positioning in orthognathic surgery. J Oral Maxillofac Surg. 1988; 46:1110–1112.
Article11. Peñarrocha MA, Peñarrocha D, Bagán JV, Peñarrocha M. Post-traumatic trigeminal neuropathy. A study of 63 cases. Med Oral Patol Oral Cir Bucal. 2012; 17:e297–e300.12. Bodéré C, Téa SH, Giroux-Metges MA, Woda A. Activity of masticatory muscles in subjects with different orofacial pain conditions. Pain. 2005; 116:33–41.
Article13. Güzel MZ, Arslan H, Klç A. Bilateral congenital trigeminal sensorimotor neuropathy presents as a severe open-bite malocclusion. J Craniofac Surg. 2006; 17:998–1001.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Implant-supported fixed prosthetic restoration using a high performance polymer (PEKK) in a mandibular unilateral resection: A case report
- PROSTHETIC REHABILITATION OF THE PARTIALLY EDENTULOUS PATIENT BY USING OSSEOINTEGRATE IMPLANT AFTER REMOVAL OF AMELOBLASTOMA
- A 20-year experience of immediate mandibular reconstruction using free fibula osteocutaneous flaps following ameloblastoma resection: Radical resection, outcomes, and recurrence
- Oral rehabilitation using implant supported fixed dental prostheses in a growing patient who underwent mandibulectomy and fibular free flap
- An esthetic appliance for the management of crown-root fracture: a case report
