Feasibility and Effectiveness of Direct Puncture and Onyx Embolization for Transverse Sinus Dural Arteriovenous Fistula
- Affiliations
-
- 1Department of Neurosurgery, Chung-Ang University Hospital, Chung-Ang University College of Medicine, Seoul, Korea.
- 2Department of Radiology, Chung-Ang University Hospital, Chung-Ang University College of Medicine, Seoul, Korea. flightdr61@hanmail.net
- 3Department of Neurosurgery, Kangwon National University School of Medicine, Chuncheon, Korea.
- KMID: 2460230
- DOI: http://doi.org/10.3349/ymj.2019.60.11.1112
Abstract
- Direct puncture and embolization of the transverse sinus (TS) for treatment of dural arteriovenous fistula (DAVF) is typically performed with coils with or without glue. We report a case of DAVF at the left TS that was treated with Onyx embolization via direct puncture of the TS. A 75-year-old woman presented with tremor, festinating gait, and dysarthria. A left TS-DAVF with retrograde superior sagittal sinus and cortical venous reflux (Cognard type IIa+b) was identified on cerebral angiography, and both TSs were occluded with thrombi. We considered that achieving complete cure by transvenous embolization via the femoral vein or transarterial embolization via occipital feeders would be difficult. Thus, we performed a small craniotomy at the occipital bone to puncture the TS. The midportion of the TS was directly punctured with a 21-G microneedle under fluoroscopic guidance. We inserted a 5-F sheath into the TS. A microcatheter was then navigated into the affected sinus. Coils were placed through the microcatheter to support Onyx formation by reducing the pressure of shunting flow. Onyx embolization was performed with the same microcatheter. The DAVF was almost completely occluded except for the presence of minimal shunting flow to the proximal TS. After 1 week, time-of-flight magnetic resonance angiography showed complete resolution of DAVF. The patient showed resolved tremor and markedly improved mental status at 1-month follow up. Direct puncture and embolization of the TS using coils and Onyx is effective and feasible method for the treatment of DAVF when other approaches seem difficult.
Keyword
MeSH Terms
Figure
-
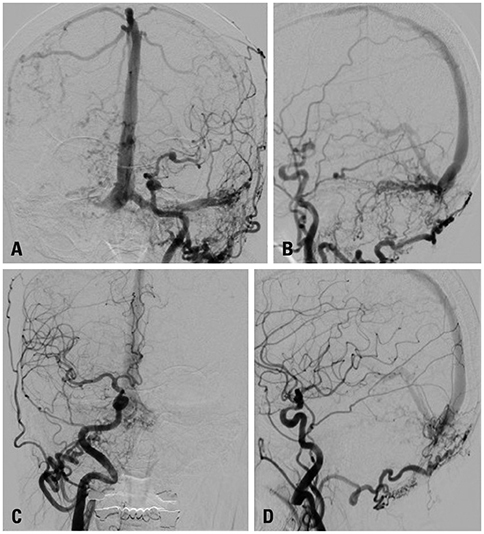
Fig. 1 Initial angiogram. (A and B) Anterior (A) and lateral (B) images of the left CCA angiogram show dural arteriovenous fistula with retrograde flow and cortical venous reflux (Cognard classification IIa+b). Diffuse numerous shunting flows are noted in the left transverse sinus. Bilateral sigmoid sinus is occluded. (C and D) Anterior (C) and lateral (D) images of right CCA angiogram show shunting flow into the torcular region. CCA, common carotid artery.
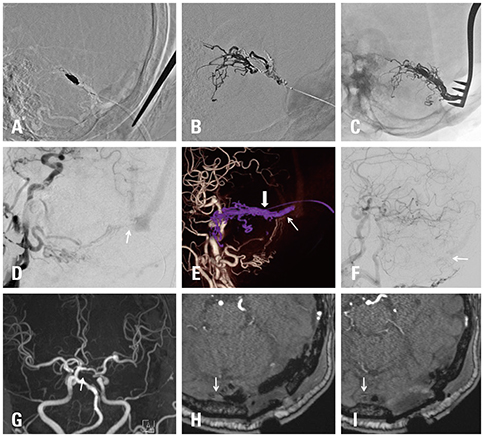
Fig. 2 Treatment and follow up. (A) Lateral image shows inserted coil mass. (B) Lateral image shows Onyx cast during embolization. (C) Lateral image shows final Onyx cast. (D and E) Left three-dimensional common carotid artery angiogram (D) and volume rendering image (E) show residual fistula from the left occipital artery in the proximal TS (arrows). Onyx refluxed over the puncture point in the left TS (thick arrow). (F) Right brachiocephalic angiogram depicts residual fistula from the right occipital artery in proximal TS (arrow). (G–I): 1-week follow-up time-of-flight magnetic resonance angiography depicts the resolution of the fistula in the proximal TS (arrows). TS, transverse sinus.
Cited by 1 articles
-
Role of surgery in management of intracranial dural arteriovenous fistulas
Young Sill Kang, Won-Sang Cho, Sung Ho Lee, Kangmin Kim, Hyun-Seung Kang, Jeong Eun Kim
J Cerebrovasc Endovasc Neurosurg. 2023;25(2):117-131. doi: 10.7461/jcen.2023.E2022.10.006.
Reference
-
1. Houdart E, Saint-Maurice JP, Chapot R, Ditchfield A, Blanquet A, Lot G, et al. Transcranial approach for venous embolization of dural arteriovenous fistulas. J Neurosurg. 2002; 97:280–286.
Article2. Cognard C, Gobin YP, Pierot L, Bailly AL, Houdart E, Casasco A, et al. Cerebral dural arteriovenous fistulas: clinical and angiographic correlation with a revised classification of venous drainage. Radiology. 1995; 194:671–680.
Article3. Duffau H, Lopes M, Janosevic V, Sichez JP, Faillot T, Capelle L, et al. Early rebleeding from intracranial dural arteriovenous fistulas: report of 20 cases and review of the literature. J Neurosurg. 1999; 90:78–84.
Article4. Bruneau M, Lubicz B, Pirotte B, Taib NO, Wikler D, Brotchi J, et al. Selective image-guided venous sinus exposure for direct embolization of dural arteriovenous fistula: technical case report. Surg Neurol. 2008; 69:192–196.
Article5. Endo S, Kuwayama N, Takaku A, Nishijima M. Direct packing of the isolated sinus in patients with dural arteriovenous fistulas of the transverse-sigmoid sinus. J Neurosurg. 1998; 88:449–456.
Article6. Liu JK, Choudhry OJ, Barnwell SL, Delashaw JB Jr, Dogan A. Single stage transcranial exposure of large dural venous sinuses for surgically-assisted direct transvenous embolization of high-grade dural arteriovenous fistulas: technical note. Acta Neurochir (Wien). 2012; 154:1855–1859.
Article7. Zink WE, Meyers PM, Connolly ES, Lavine SD. Combined surgical and endovascular management of a complex posttraumatic dural arteriovenous fistula of the tentorium and straight sinus. J Neuroimaging. 2004; 14:273–276.
Article8. Caplan JM, Kaminsky I, Gailloud P, Huang J. A single burr hole approach for direct transverse sinus cannulation for the treatment of a dural arteriovenous fistula. BMJ Case Rep. 2014; 2014:bcr2013011011.
Article9. Matsuzaki J, Kono K, Umesaki A, Kashimura Y, Matsumoto H, Terada T. [Transvenous embolization by direct puncture of the superior sagittal sinus using indocyanine green (ICG) videoangiography for treatment of dural arteriovenous fistula of the transverse-sigmoid sinus: a case report]. No Shinkei Geka. 2017; 45:591–598.10. Mickle JP, Quisling RG. The transtorcular embolization of vein of Galen aneurysms. J Neurosurg. 1986; 64:731–735.
Article11. Zhang Y, Li Q, Huang QH. Embolization of a superior sagittal sinus dural arteriovenous fistula under intrasinus balloon protection: a case report. Interv Neuroradiol. 2015; 21:94–100.
Article12. Watanabe J, Maruya J, Nishimaki K, Ito Y. Onyx removal after embolization of a superior sagittal sinus dural arteriovenous fistula involving scalp artery. Surg Neurol Int. 2016; 7:Suppl 14. S410–S414.
Article13. Rabinov JD, Yoo AJ, Ogilvy CS, Carter BS, Hirsch JA. ONYX versus n-BCA for embolization of cranial dural arteriovenous fistulas. J Neurointerv Surg. 2013; 5:306–310.
Article14. Akin ED, Perkins E, Ross IB. Surgical handling characteristics of an ethylene vinyl alcohol copolymer compared with N-butyl cyanoacrylate used for embolization of vessels in an arteriovenous malformation resection model in swine. J Neurosurg. 2003; 98:366–370.
Article15. Murayama Y, Viñuela F, Ulhoa A, Akiba Y, Duckwiler GR, Gobin YP, et al. Nonadhesive liquid embolic agent for cerebral arteriovenous malformations: preliminary histopathological studies in swine rete mirabile. Neurosurgery. 1998; 43:1164–1175.
Article16. Torok CM, Nogueira RG, Yoo AJ, Leslie-Mazwi TM, Hirsch JA, Stapleton CJ, et al. Transarterial venous sinus occlusion of dural arteriovenous fistulas using ONYX. Interv Neuroradiol. 2016; 22:711–716.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Dural Arteriovenous Fistula Involving Transverse Sinus: Successful Embolization Using Onyx(R)
- Transcranial Direct Middle Meningeal Artery Puncture for the Onyx Embolization of Dural Arteriovenous Fistula Involving the Superior Sagittal Sinus
- Dural Arteriovenous Fistula Involving an Isolated Sinus Treated Using Transarterial Onyx Embolization
- Infantile Dural Arteriovenous Fistula of the Transverse Sinus Presenting with Ocular Symptoms, Case Reports and Review of Literature
- Transvenous injection of n-butyl 2-cyanoacrylate to obliterate the pathologic cavernous sinus as a salvage technique for incompletely obliterated complex cavernous sinus dural arteriovenous fistula after transvenous coil embolization
