Bone Flap Changes after Cranioplasty Using Frozen Autologous Bone Flaps: A Three-Dimensional Volumetric Reconstruction Study
- Affiliations
-
- 1Department of Neurosurgery, Pusan National University Hospital, Busan, Korea.
- 2Catholic Neuroscience Center, Department of Neurosurgery, St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. chough@catholic.ac.kr
- 3Department of Neurosurgery, Pusan National University Yangsan Hospital, Yangsan, Korea.
- KMID: 2460224
- DOI: http://doi.org/10.3349/ymj.2019.60.11.1067
Abstract
- PURPOSE
Bone flap resorption (BFR) after cranioplasty with an autologous bone flap (ABF) is well known. However, the prevalences and degrees of BFR remain unclear. This study aimed to evaluate changes in ABFs following cranioplasty and to investigate factors related with BFR.
MATERIALS AND METHODS
We retrospectively reviewed 97 patients who underwent cranioplasty with frozen ABF between January 2007 and December 2016. Brain CT images of these patients were reconstructed to form three-dimensional (3D) images, and 3D images of ABF were separated using medical image editing software. ABF volumes on images were measured using 3D image editing software and were compared between images in the immediate postoperative period and at postoperative 12 months. Risk factors related with BFR were also analyzed.
RESULTS
The volumes of bone flaps calculated from CT images immediately after cranioplasty ranged from 55.3 cm³ to 175 cm³. Remnant bone flap volumes at postoperative 12 months ranged from 14.2% to 102.5% of the original volume. Seventy-five patients (77.3%) had a BFR rate exceeding 10% at 12 months after cranioplasty, and 26 patients (26.8%) presented severe BFR over 40%. Ten patients (10.3%) underwent repeated cranioplasty due to severe BFR. The use of a 5-mm burr for central tack-up sutures was significantly associated with BFR (p<0.001).
CONCLUSION
Most ABFs after cranioplasty are absorbed. Thus, when using frozen ABF, patients should be adequately informed. To prevent BFR, making holes must be kept to a minimum during ABF grafting.
MeSH Terms
Figure
-
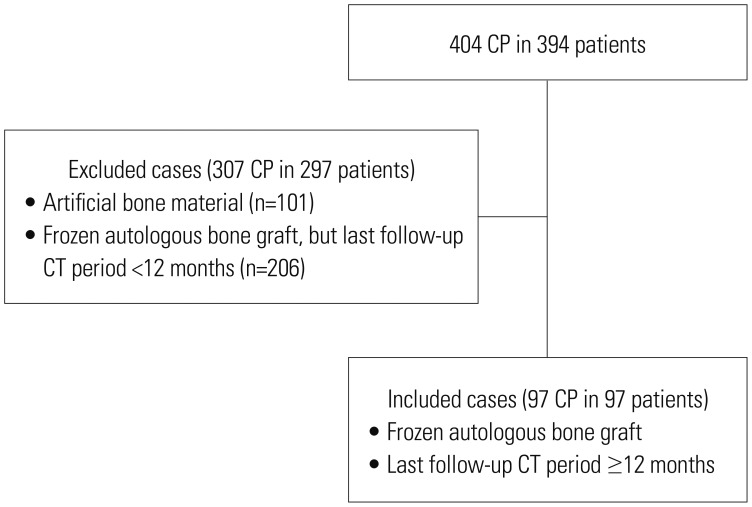
Fig. 1 Flowchart of cases included in or excluded from the study. CP, cranioplasty.
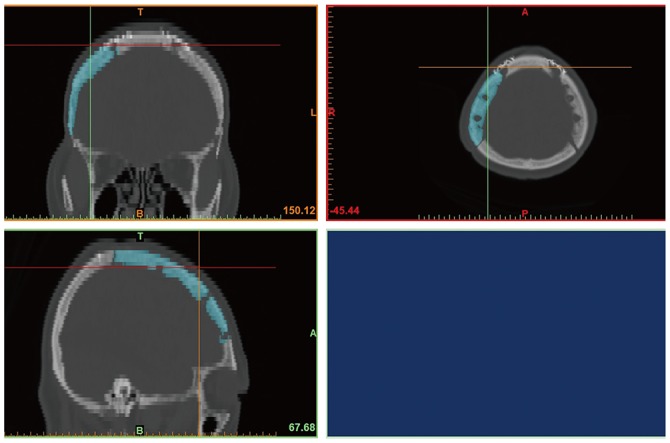
Fig. 2 Volume measurement with 3D modeling software. Using Materialise Mimics, we selected autologous bone flaps from CT scans of the skull and reconstructed them into 3D images. The reconstructed images were converted into STL files for 3D images. The STL file of the bone flap was imported by Netfabb to calculate the volume. 3D, three dimensional; STL, stereolithography.
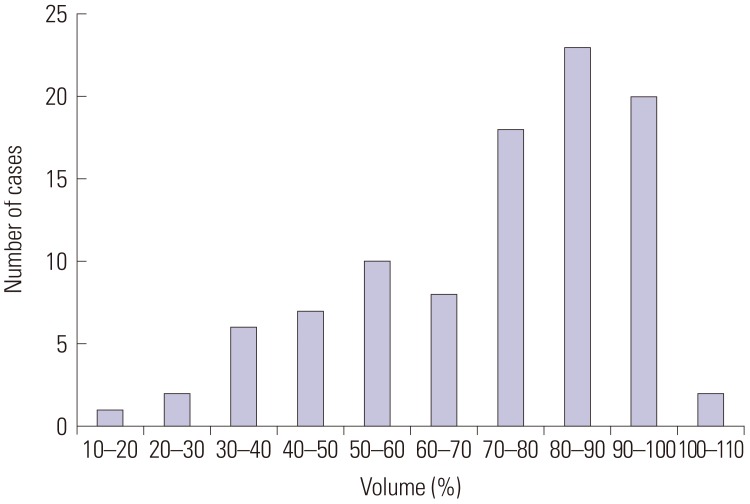
Fig. 3 Distribution of volumes of remnant bone flap.
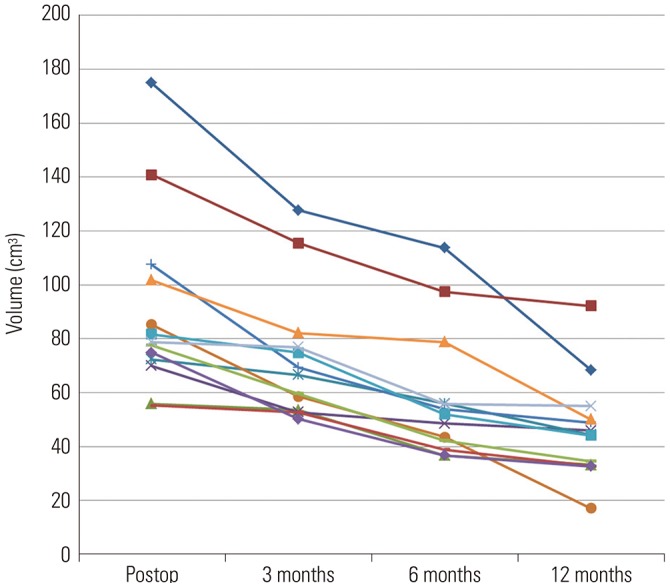
Fig. 4 Changes in volume of ABF of 13 patients with serial computed tomography scans at 3, 6, and 12 months in the bone flap resorption group. On average, the volume of ABF at 12 months was preserved by an average of 52.1%. ABF, autologous bone flap.
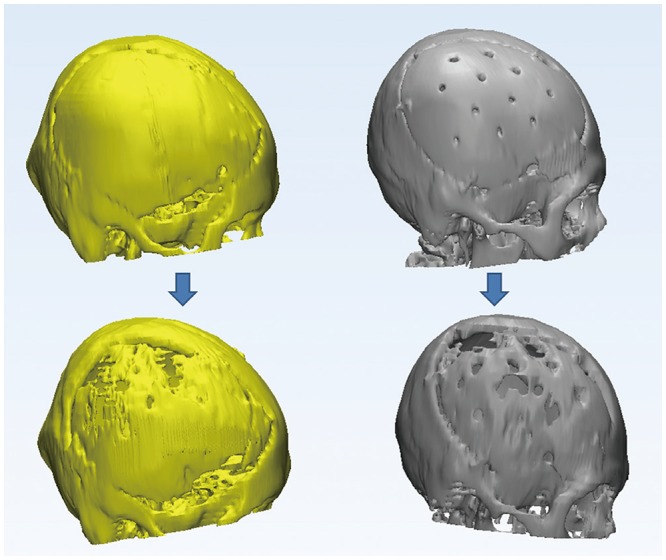
Fig. 5 Changes in the skull and ABF after cranioplasty in the BFR group. In general, BFR began in the parietal bone and the temporal bone (left). If wide holes existed on ABF, BFR was also initiated at the holes (right). ABF, autologous bone flap; BFR, bone flap resorption.
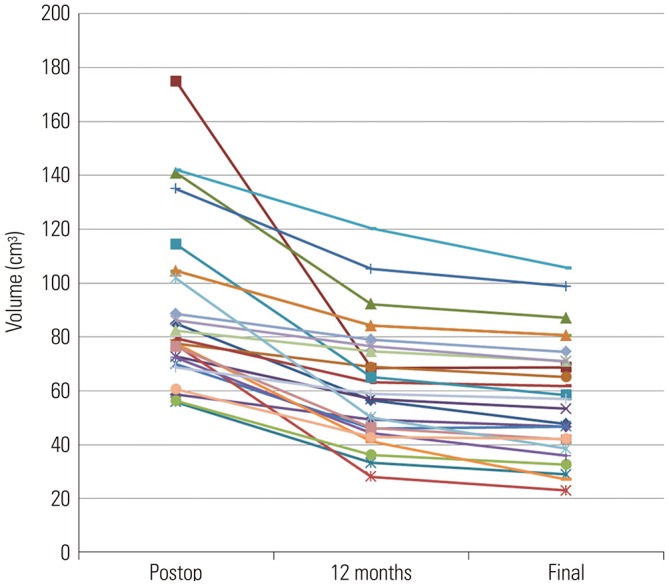
Fig. 6 Changes in the volume of ABF after 12 months in the bone flap resorption group. Unlike before 12 months, the decline decreased after 12 months. After an additional 12 months, the volume of ABF decreased only by an average of 5.8%. ABF, autologous bone flap.
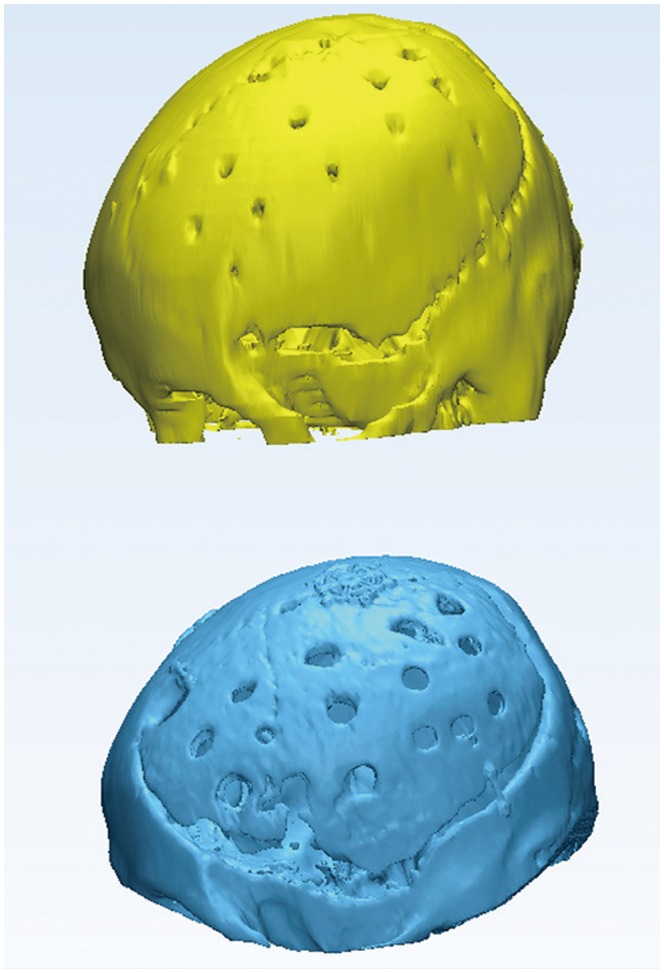
Fig. 7 Three-dimensional images of the cranium following cranioplasty. The upper image was obtained from immediate postoperative CT scans, and the lower image was obtained from CT scans at 12 months after surgery. The volume of the remaining autologous bone flap was 67% of its original volume, and repeated cranioplasty was performed due to appearance issues that caused depression in the forehead area.
Reference
-
1. Hofmeijer J, Kappelle LJ, Algra A, Amelink GJ, van Gijn J, van der Worp HB. HAMLET investigators. Surgical decompression for space-occupying cerebral infarction (the Hemicraniectomy After Middle Cerebral Artery infarction with Life-threatening Edema Trial [HAMLET]): a multicentre, open, randomised trial. Lancet Neurol. 2009; 8:326–333. PMID: 19269254.
Article2. Fisher CM, Ojemann RG. Bilateral decompressive craniectomy for worsening coma in acute subarachnoid hemorrhage. Observations in support of the procedure. Surg Neurol. 1994; 41:65–74. PMID: 8310390.
Article3. Guerra WK, Gaab MR, Dietz H, Mueller JU, Piek J, Fritsch MJ. Surgical decompression for traumatic brain swelling: indications and results. J Neurosurg. 1999; 90:187–196. PMID: 9950487.
Article4. Honeybul S, Ho KM. How “successful” is calvarial reconstruction using frozen autologous bone? Plast Reconstr Surg. 2012; 130:1110–1117. PMID: 23096611.
Article5. Dujovny M, Fernandez P, Alperin N, Betz W, Misra M, Mafee M. Post-cranioplasty cerebrospinal fluid hydrodynamic changes: magnetic resonance imaging quantitative analysis. Neurol Res. 1997; 19:311–316. PMID: 9192385.
Article6. Winkler PA, Stummer W, Linke R, Krishnan KG, Tatsch K. Influence of cranioplasty on postural blood flow regulation, cerebrovascular reserve capacity, and cerebral glucose metabolism. J Neurosurg. 2000; 93:53–61.
Article7. Honeybul S. Decompressive craniectomy: a new complication. J Clin Neurosci. 2009; 16:727–729. PMID: 19261473.
Article8. Iwama T, Yamada J, Imai S, Shinoda J, Funakoshi T, Sakai N. The use of frozen autogenous bone flaps in delayed cranioplasty revisited. Neurosurgery. 2003; 52:591–596. PMID: 12590683.
Article9. Kim JS, Cheong JH, Ryu JI, Kim JM, Kim CH. Bone flap resorption following cranioplasty after decompressive craniectomy: preliminary report. Korean J Neurotrauma. 2015; 11:1–5. PMID: 27169057.
Article10. Park SP, Kim JH, Kang HI, Kim DR, Moon BG, Kim JS. Bone flap resorption following cranioplasty with autologous bone: quantitative measurement of bone flap resorption and predictive factors. J Korean Neurosurg Soc. 2017; 60:749–754. PMID: 29142636.11. Grant GA, Jolley M, Ellenbogen RG, Roberts TS, Gruss JR, Loeser JD. Failure of autologous bone-assisted cranioplasty following decompressive craniectomy in children and adolescents. J Neurosurg. 2004; 100(2 Suppl Pediatrics):163–168. PMID: 14758944.
Article12. Lee JH, Han IH, Choi BK, Nam KH, Kim DH, Lee CS. Virtual preoperative simulation for excision of spinal tumors: surgeon processing of medical computer-assisted design software. Korean J Spine. 2017; 14:170–174. PMID: 29301180.
Article13. Vanaclocha V, Sáiz-Sapena N, García-Casasola C, De Alava E. Cranioplasty with autogenous autoclaved calvarial bone flap in the cases of tumoural invasion. Acta Neurochir (Wien). 1997; 139:970–976. PMID: 9401658.
Article14. Lee SH, Yoo CJ, Lee U, Park CW, Lee SG, Kim WK. Resorption of autogenous bone graft in cranioplasty: resorption and reintegration failure. Korean J Neurotrauma. 2014; 10:10–14. PMID: 27169026.
Article15. Osawa M, Hara H, Ichinose Y, Koyama T, Kobayashi S, Sugita Y. Cranioplasty with a frozen and autoclaved bone flap. Acta Neurochir (Wien). 1990; 102:38–41. PMID: 2305650.
Article16. Prolo DJ, Oklund SA. Composite autogeneic human cranioplasty: frozen skull supplemented with fresh iliac corticocancellous bone. Neurosurgery. 1984; 15:846–851. PMID: 6514157.
Article17. Dünisch P, Walter J, Sakr Y, Kalff R, Waschke A, Ewald C. Risk factors of aseptic bone resorption: a study after autologous bone flap reinsertion due to decompressive craniotomy. J Neurosurg. 2013; 118:1141–1147. PMID: 23451904.
Article18. Brommeland T, Rydning PN, Pripp AH, Helseth E. Cranioplasty complications and risk factors associated with bone flap resorption. Scand J Trauma Resusc Emerg Med. 2015; 23:75. PMID: 26437934.
Article19. Schwarz F, Dünisch P, Walter J, Sakr Y, Kalff R, Ewald C. Cranioplasty after decompressive craniectomy: is there a rationale for an initial artificial bone-substitute implant? A single-center experience after 631 procedures. J Neurosurg. 2016; 124:710–715. PMID: 26406796.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Analysis of Cranioplasty Using Frozen Autologous Bone Following Post-Traumatic Decompressive Craniectomy
- Analyses Using Micro-CT Scans and Tissue Staining on New Bone Formation and Bone Fusion According to the Timing of Cranioplasty via Frozen Autologous Bone Flaps in Rabbits : A Preliminary Report
- Erratum to “Bone Flap Changes after Cranioplasty Using Frozen Autologous Bone Flaps: A Three-Dimensional Volumetric Reconstruction Study” by Lee JH, et al. (Yonsei Med J 2019 Nov;60(11):1067-1073)
- Cranioplasty Using Frozen Autologous Bone
- Clinical Outcomes of Cranioplasty Using a Customized Artificial Bone Flap Made by a 3D Printing Technique
