Spontaneous Intracranial Vertebral Artery Dissection in a 2-Year-Old Child Diagnosed with High-Resolution MRI: a Case Report
- Affiliations
-
- 1Department of Radiology, Ajou University School of Medicine, Ajou University Medical Center, Suwon, Korea. miranhanajou@gmail.com
- 2Department of Pediatrics, Ajou University School of Medicine, Ajou University Medical Center, Suwon, Korea.
- KMID: 2459880
- DOI: http://doi.org/10.13104/imri.2019.23.3.259
Abstract
- Although many imaging modalities can play some roles in the diagnosis of vertebral artery dissection (VAD), digital subtraction angiography (DSA) remains the gold standard method, with the highest detection rate and ability to assist in planning for endovascular treatment. However, this tool is often avoided in children because its invasive nature and it exposes them to radiation. High resolution magnetic resonance imaging (HR-MRI) have been suggested to be a reliable and non-invasive alternative, but it has never been discussed in children in whom vertebral artery dissection is a rare condition. In this report, we evaluate a case of a 2-year-old child who initially presented with cerebellar symptoms, and was early diagnosed with vertebral artery dissection using HR-MRI and was successfully treated.
MeSH Terms
Figure
-
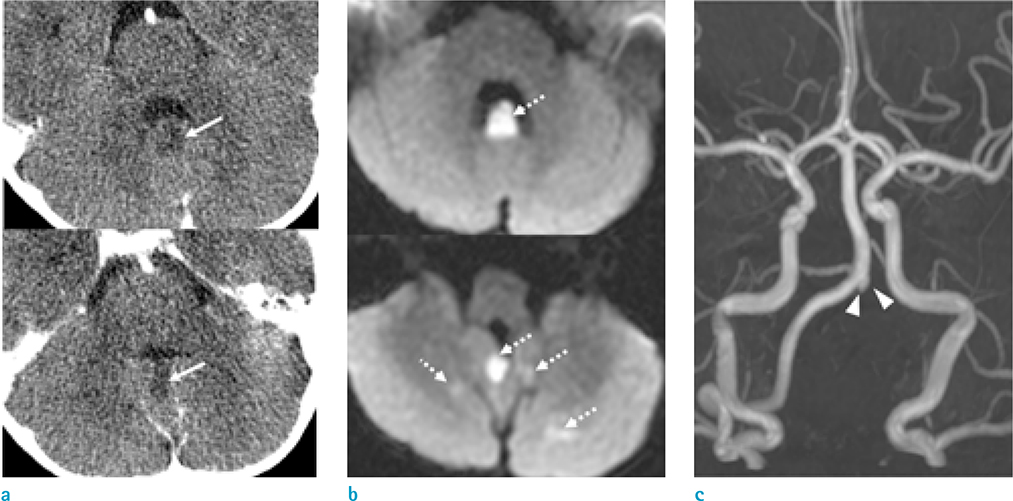
Fig. 1 A 2-year-old boy underwent CT and MRI due to sudden onset of irritability, vomiting and gait disturbance. Focal low density (arrows) is noted at cerebellar vermis on the initial CT scan (a) and diffusion restriction foci (dashed arrows) are observed at the corresponding cerebellar vermis and additionally at posterior inferior cerebellar artery (PICA) territory on DWI (b). On the MRA, the left vertebral artery flow is not seen and sharp distal edge is observed (c, arrowheads)
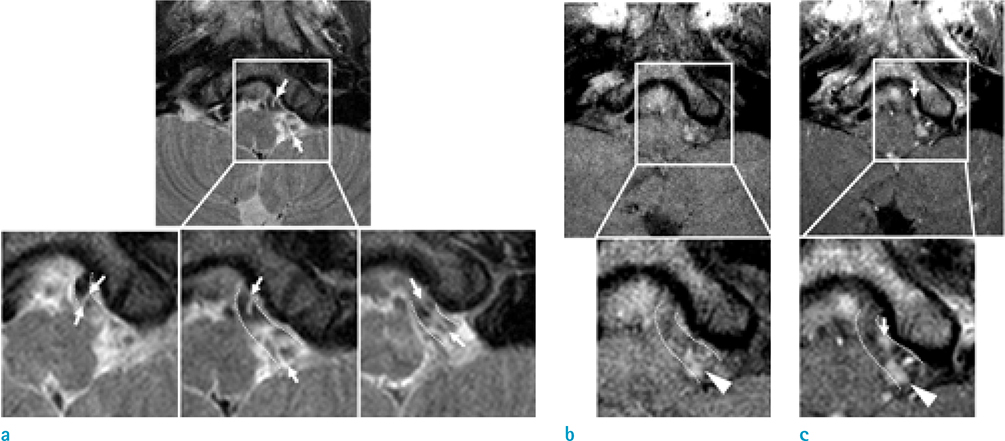
Fig. 2 High resolution MRI (HR-MRI) was performed 5 days later after the onset of the symptoms to confirm the vertebral artery dissection. The dilatation of the outer wall (dashed line) at occluded left vertebral artery segment on MRA is seen on T2WI (a) of HR-MRI. The dissection flap (arrows points to both ends of flap on each slice) is also evident on serial T2WIs (from left to right in figure show cranio-caudal slices). The mural hematoma (arrowheads) in early subacute stage is detectable as high signal intensity lesion on not only T1WI (b) but also contrast enhanced (CE)-T1WI (c) at medial side of double lumen. The dissection flap is also enhanced linearly (arrow) on CE-T1WI.

Fig. 3 Follow up HR-MRI was performed 3-months later. Normalized vascular flow (arrows) and contour (thick dashed lines) of left vertebral artery are seen on MRA (a), HR-T2WI (b) and T1WI (c). The dissection flap and hematoma are no longer visible. The left PICA artery flow (dashed arrows) and vascular contour (thin dashed line, thin dashed circle indicates the origin of left PICA from vertebral artery) are also newly observed on follow up images.
Reference
-
1. Hasan I, Wapnick S, Tenner MS, Couldwell W. Vertebral artery dissection in children: a comprehensive review. Pediatr Neurosurg. 2002; 37:168–177.
Article2. Cheon JE, Kim IO, Kim WS, Hwang YS, Wang KC, Yeon KM. MR diagnosis of cerebellar infarction due to vertebral artery dissection in children. Pediatr Radiol. 2001; 31:163–166.
Article3. Rafay MF, Armstrong D, Deveber G, Domi T, Chan A, MacGregor DL. Craniocervical arterial dissection in children: clinical and radiographic presentation and outcome. J Child Neurol. 2006; 21:8–16.
Article4. Han M, Rim NJ, Lee JS, Kim SY, Choi JW. Feasibility of high-resolution MR imaging for the diagnosis of intracranial vertebrobasilar artery dissection. Eur Radiol. 2014; 24:3017–3024.
Article5. Kaufmann TJ, Huston J 3rd, Mandrekar JN, Schleck CD, Thielen KR, Kallmes DF. Complications of diagnostic cerebral angiography: evaluation of 19,826 consecutive patients. Radiology. 2007; 243:812–819.6. Choi YJ, Jung SC, Lee DH. Vessel wall imaging of the intracranial and cervical carotid arteries. J Stroke. 2015; 17:238–255.
Article7. Habs M, Pfefferkorn T, Cyran CC, et al. Age determination of vessel wall hematoma in spontaneous cervical artery dissection: a multi-sequence 3T cardiovascular magnetic resonance study. J Cardiovasc Magn Reson. 2011; 13:76.
Article8. Park KJ, Jung SC, Kim HS, et al. Multi-contrast high-resolution magnetic resonance findings of spontaneous and unruptured intracranial vertebral artery dissection: qualitative and quantitative analysis according to stages. Cerebrovasc Dis. 2016; 42:23–31.
Article9. Mizutani T. Natural course of intracranial arterial dissections. J Neurosurg. 2011; 114:1037–1044.
Article10. Tan MA, Armstrong D, MacGregor DL, Kirton A. Late complications of vertebral artery dissection in children: pseudoaneurysm, thrombosis, and recurrent stroke. J Child Neurol. 2009; 24:354–360.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- High-Resolution Magnetic Resonance Imaging of Intracranial Vertebral Artery Dissecting Aneurysm for Planning of Endovascular Treatment
- Chirotherapy Associated Vertebral Artery Dissection: Case Illustration and Literature Review
- Spontaneous Resolution of Dissecting Aneurysm of the Vertebral Artery
- A Case of Bilateral Spontaneous Extracranial Vertebral Artery Dissection
- Diagnosis and Management of the Spontaneous Intracranial Vertebral Artery Dissection
