Technical feasibility of da Vinci SP single-port robotic cholecystectomy: a case report
- Affiliations
-
- 1Department of Surgery, Ospital ng Makati, Metro Manila, Philippines.
- 2Liver and Pancreas Center, The Medical City-Clark, Clark Freeport Zone, Philippines.
- 3Division of HBP Surgery, Department of Surgery, Yonsei University College of Medicine, Seoul, Korea. cmkang@yuhs.ac
- 4Pancreatobiliary Cancer Center, Yonsei Cancer Center, Severance Hospital, Seoul, Korea.
- KMID: 2459320
- DOI: http://doi.org/10.4174/astr.2019.97.4.217
Abstract
- The da Vinci surgical system released its new pure single-port platform, the da Vinci SP, offering improvements and refinements for established robotic single-site procedures. Herein, we present the first case of robotic single-site cholecystectomy using the da Vinci SP system (RSPC) demonstrating its safety and technical feasibility. A 59-year-old female with chronic calculus cholecystitis was admitted for elective RSPC. Docking time took 6 minutes. The patient underwent successful RSPC with a total operation time of 89 minutes. There was no significant intraoperative event. The patient had unremarkable postoperative course. Multijoint instruments, simple docking process, and third-arm functionality are among the RSPC's advantages. Absence of the port for an assistant surgeon can be a hindrance in performing more complicated surgeries. The present case suggests that RSPC is safe and feasible. The promising features and potential application of da Vinci SP in hepatobiliary and pancreas surgery need further study.
Keyword
Figure
-
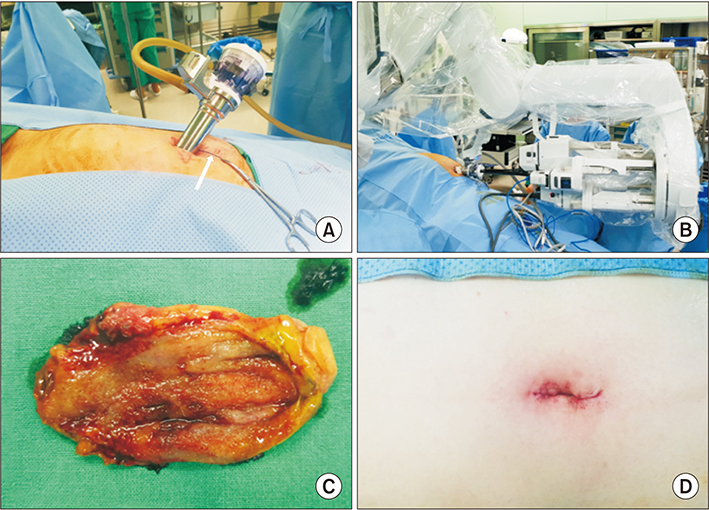
Fig. 1 Intraoperative view. Pure single port placed through a 2.5-cm umbilical incision, for accommodating 4 instruments including camera with extra orifice for assist port. Note no additional port for assist surgeon's intervention. (A) Endo-pouch and 2 gauzes were put into the abdominal cavity before robot docking (white arrow). (B) External view of the docked da Vinci SP. Three arms and one endoscope entering the single-port parallel to each other. Surgical specimen with small gallbladder stones (C), and 2.5-cm skin incision at the umbilicus (D).
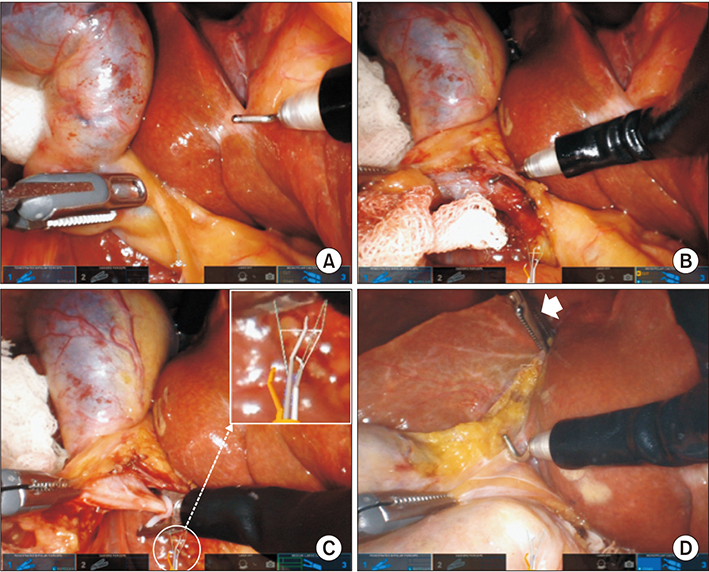
Fig. 2 Monitor view during cholecystectomy. Left grasper controlled by nondominant left hand. Dominant right hand controls the hook. Left hand can swap to control the 3rd arm grasper by stepping on the switch control pedal for retracting gallbladder toward upward and lateral direction (A). Cystic duct isolation (B) cystic duct clipping. Note the new graphic user interface in the lower middle part of the display (magnification showed) in the surgeon console which shows the real-time relationship of 4 instruments (C). Note the effective 3rd arm movement (white arrow, D).
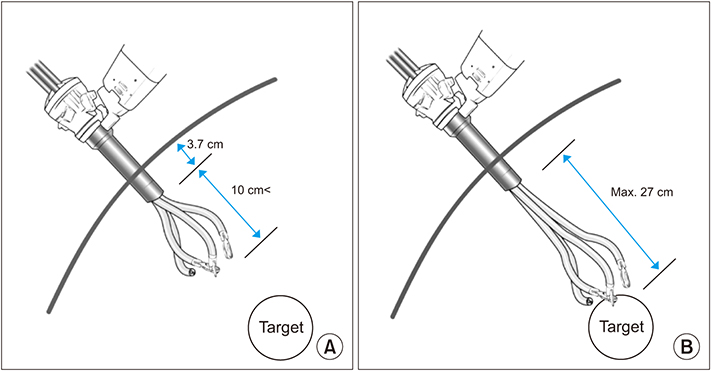
Fig. 3 (A) According to the mechanical concept of SP robotic surgical system, target lesions should be at least 15 cm apart from the entry site of single port. If the lesion is expected to be closer than this range, another port system will be required for system moving backward. (B) Maximum distance that robotic instruments can reach is estimated to be 27 cm from the outlet of single port.
Cited by 1 articles
-
ArtiSential laparoscopic cholecystectomy: a comparative analysis with robotic single-port cholecystectomy
Seoung Yoon Rho, Munseok Choi, Sung Hyun Kim, Seung Soo Hong, Brian Kim Poh Goh, Yuichi Nagakawa, Minoru Tanabe, Daisuke Asano, Chang Moo Kang
Ann Surg Treat Res. 2024;107(6):336-345. doi: 10.4174/astr.2024.107.6.336.
Reference
-
1. Lanfranco AR, Castellanos AE, Desai JP, Meyers WC. Robotic surgery: a current perspective. Ann Surg. 2004; 239:14–21.2. Leung T, Vyas D. Robotic surgery: applications. Am J Robot Surg. 2014; 1:1–64.
Article3. Kang CM, Chi HS, Hyeung WJ, Kim KS, Choi JS, Lee WJ, et al. The first Korean experience of telemanipulative robot-assisted laparoscopic cholecystectomy using the da Vinci system. Yonsei Med J. 2007; 48:540–545.
Article4. Qadan M, Curet MJ, Wren SM. The evolving application of single-port robotic surgery in general surgery. J Hepatobiliary Pancreat Sci. 2014; 21:26–33.
Article5. Lee SH, Jung MJ, Hwang HK, Kang CM, Lee WJ. The first experiences of robotic single-site cholecystectomy in Asia: a potential way to expand minimally-invasive single-site surgery. Yonsei Med J. 2015; 56:189–195.
Article6. Wren SM, Curet MJ. Single-port robotic cholecystectomy: results from a first human use clinical study of the new da Vinci single-site surgical platform. Arch Surg. 2011; 146:1122–1127.7. Pietrabissa A, Sbrana F, Morelli L, Badessi F, Pugliese L, Vinci A, et al. Overcoming the challenges of single-incision cholecystectomy with robotic single-site technology. Arch Surg. 2012; 147:709–714.
Article8. Bertolo R, Garisto J, Gettman M, Kaouk J. Novel system for robotic single-port surgery: feasibility and state of the art in urology. Eur Urol Focus. 2018; 4:669–673.
Article9. Hwang HK, Choi SH, Kang CM, Lee WJ. Single-fulcrum laparoscopic cholecystectomy in uncomplicated gallbladder diseases: a retrospective comparative analysis with conventional laparoscopic cholecystectomy. Yonsei Med J. 2013; 54:1471–1477.
Article10. Jung MJ, Lee SY, Lee SH, Kang CM, Lee WJ. Single-site robotic cholecystectomy: reverse-port technique. Medicine (Baltimore). 2015; 94:e1871.11. Chong JU, Kang CM. Robotic single-site plus one port: pancreas enucleation. J Gastrointest Surg. 2019; 23:1527–1528.
Article12. Han HJ, Kang CM. Reduced port minimally invasive distal pancreatectomy: single-port laparoscopic versus robotic single-site plus one-port distal pancreatectomy. Surg Endosc. 2019; 33:1091–1099.
Article13. Kim SH, Kang CM, Lee WJ. Robotic single-site plus one port distal pancreatectomy. Surg Endosc. 2017; 31:4258–4259.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Single-Port Transaxillary Robotic Thyroidectomy (START) for Benign Thyroid Tumors
- Initial Clinical Experience of Pure Single-Incision Robotic Right Hemicolectomy with da Vinci SP Platform
- Da Vinci SP Single-Port Robotic Surgery in Gynecologic Tumors: Single Surgeon’s Initial Experience with 100 Cases
- Single-Port Transaxillary Robotic Bilateral Total Thyroidectomy (START) for Graves’ Disease: First Initial 10 Cases Using da Vinci SP Robotic System
- Robotic single-port plus one-port splenic vessel-conserving spleen-preserving distal pancreatectomy: a case report
