Incarcerated Hiatal Hernia with Perforation after Laparoscopic Total Gastrectomy with Roux-en-Y Reconstruction: a Case Report
- Affiliations
-
- 1Department of Surgery, Division of General Surgery, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan (R.O.C.). khho@vghks.gov.tw
- KMID: 2458825
- DOI: http://doi.org/10.5230/jgc.2019.19.e7
Abstract
- The occurrence of hiatal hernia after total gastrectomy with Roux-en-Y reconstruction is rare. We report the case of a 76-year-old man who presented with dyspnea, vomiting, and fever around 8 days after total gastrectomy with Roux-en-Y reconstruction. Abdominal computed tomography revealed a hiatal hernia containing part of the small intestine in the left thoracic cavity. Emergent reduction and repair of the hiatal hernia were performed later. Operative findings revealed that the Roux limb was incarcerated in the left pleural cavity. Esophagojejunostomy leakage, perforation of the small intestine with transient ischemic change, and pyothorax were also found. Thus, feeding jejunostomy, thoracoscopic decortication, and diversion T-tube esophagostomy were performed. Considering that the main cause of hiatal hernia is blunt dissection with division of the phrenoesophageal membrane, approximating the crus with 1 or 2 figure-8 sutures, according to the size of the defect, to prevent the incidence of hiatal hernia after total gastrectomy may be performed.
Keyword
MeSH Terms
Figure
-
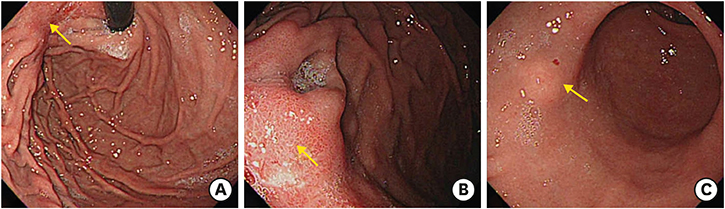
Fig. 1 Preoperative upper gastrointestinal panendoscopy. (A, B) The arrow indicates the hyperemic area at the posterior wall of the high body to the cardia. (C) The arrow indicates the submucosal mass at the lesser curvature side of the antrum. No preoperative hiatal hernia was observed.

Fig. 2 (A) Pre- and (B) post-gastrectomy hiatus.

Fig. 3 (A) Chest radiograph showing the intestine in the left lung field. (B) Abdominal computed tomography image showing distended loops of the small intestine in the left thoracic cavity.
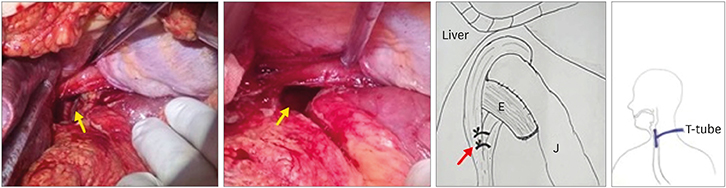
Fig. 4 Intraoperative finding showing the orifice of the hernia (yellow arrow). The red arrow indicates the crural approximation.
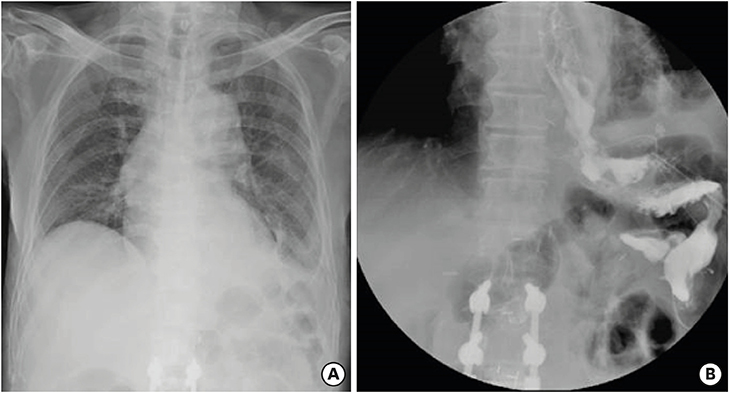
Fig. 5 (A) The latest chest radiograph. (B) The latest esophagogram showing no recurrent hiatal hernia before hospital discharge.
Reference
-
1. Ghahremani GG. Internal abdominal hernias. Surg Clin North Am. 1984; 64:393–406.
Article2. Miyagaki H, Takiguchi S, Kurokawa Y, Hirao M, Tamura S, Nishida T, et al. Recent trend of internal hernia occurrence after gastrectomy for gastric cancer. World J Surg. 2012; 36:851–857.
Article3. Aoki M, Saka M, Morita S, Fukagawa T, Katai H. Afferent loop obstruction after distal gastrectomy with Roux-en-Y reconstruction. World J Surg. 2010; 34:2389–2392.
Article4. Gayer G, Barsuk D, Hertz M, Apter S, Zissin R. CT diagnosis of afferent loop syndrome. Clin Radiol. 2002; 57:835–839.
Article5. Yi HW, Kim SM, Kim SH, Shim JH, Choi MG, Lee JH, et al. Complications leading reoperation after gastrectomy in patients with gastric cancer: frequency, type, and potential causes. J Gastric Cancer. 2013; 13:242–246.
Article6. Paroz A, Calmes JM, Giusti V, Suter M. Internal hernia after laparoscopic Roux-en-Y gastric bypass for morbid obesity: a continuous challenge in bariatric surgery. Obes Surg. 2006; 16:1482–1487.
Article7. Steele KE, Prokopowicz GP, Magnuson T, Lidor A, Schweitzer M. Laparoscopic antecolic Roux-en-Y gastric bypass with closure of internal defects leads to fewer internal hernias than the retrocolic approach. Surg Endosc. 2008; 22:2056–2061.
Article8. Larkin JO, Cooke F, Ravi N, Reynolds JV. Internal hernia following total gastrectomy with Roux-en-Y reconstruction. Ann R Coll Surg Engl. 2011; 93:e71–e73.
Article9. Balázs A, Forgács A, Flautner L, Kupcsulik P. A case of unusual complication of diaphragmatic herniation of transverse colon following transhiatal esophagectomy. Orv Hetil. 1997; 138:2535–2538.10. Aly A, Watson DI. Diaphragmatic hernia after minimally invasive esophagectomy. Dis Esophagus. 2004; 17:183–186.
Article11. Price TN, Allen MS, Nichols FC 3rd, Cassivi SD, Wigle DA, Shen KR, et al. Hiatal hernia after esophagectomy: analysis of 2,182 esophagectomies from a single institution. Ann Thorac Surg. 2011; 92:2041–2045.
Article12. Tashiro Y, Murakami M, Otsuka K, Saito K, Saito A, Motegi K, et al. Intrathoracic hernia after total gastrectomy. Case Rep Gastroenterol. 2016; 10:1–6.
Article13. Hamaloglu E, Topaloglu S, Törer N. Diaphragmatic herniation after transhiatal esophagectomy. Dis Esophagus. 2002; 15:186–188.
Article14. van Sandick JW, Knegjens JL, van Lanschot JJ, Obertop H. Diaphragmatic herniation following oesophagectomy. Br J Surg. 1999; 86:109–112.
Article15. Choi YU, North JH Jr. Diaphragmatic hernia after Ivor-Lewis esophagectomy manifested as lower gastrointestinal bleeding. Am Surg. 2001; 67:30–32.16. Sasako M, Sano T, Yamamoto S, Sairenji M, Arai K, Kinoshita T, et al. Left thoracoabdominal approach versus abdominal-transhiatal approach for gastric cancer of the cardia or subcardia: a randomised controlled trial. Lancet Oncol. 2006; 7:644–651.
Article17. Bracale U, Marzano E, Nastro P, Barone M, Cuccurullo D, Cutini G, et al. Side-to-side esophagojejunostomy during totally laparoscopic total gastrectomy for malignant disease: a multicenter study. Surg Endosc. 2010; 24:2475–2479.
Article18. Gong CS, Kim BS, Kim HS. Comparison of totally laparoscopic total gastrectomy using an endoscopic linear stapler with laparoscopic-assisted total gastrectomy using a circular stapler in patients with gastric cancer: a single-center experience. World J Gastroenterol. 2017; 23:8553–8561.
Article19. Santos Bdo N, de Oliveira MB, Peixoto RD. Hiatal hernia as a total gastrectomy complication. Case Rep Oncol. 2016; 9:100–105.
Article20. Iannelli A, Facchiano E, Gugenheim J. Internal hernia after laparoscopic Roux-en-Y gastric bypass for morbid obesity. Obes Surg. 2006; 16:1265–1271.
Article21. Comeau E, Gagner M, Inabnet WB, Herron DM, Quinn TM, Pomp A. Symptomatic internal hernias after laparoscopic bariatric surgery. Surg Endosc. 2005; 19:34–39.
Article22. Coleman MH, Awad ZT, Pomp A, Gagner M. Laparoscopic closure of the Petersen mesenteric defect. Obes Surg. 2006; 16:770–772.
Article23. Bauman RW, Pirrello JR. Internal hernia at Petersen's space after laparoscopic Roux-en-Y gastric bypass: 6.2% incidence without closure--a single surgeon series of 1047 cases. Surg Obes Relat Dis. 2009; 5:565–570.
Article24. Miyashiro LA, Fuller WD, Ali MR. Favorable internal hernia rate achieved using retrocolic, retrogastric alimentary limb in laparoscopic Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2010; 6:158–162.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Laparoscopic Hiatal Hernia Repair and Roux-en-Y Conversion for Refractory Duodenogastroesophageal Reflux after Billroth I Distal Gastrectomy
- A Peterson's hernia and subsequent small bowel volvulus: surgical reconstruction utilizing transverse colon as a new Roux-en-Y limb - 1 case
- Laparoscopic Hiatal Hernia Repair during Laparoscopic Roux-en-Y Gastric Bypass (LRYGB)
- Esophageal Hiatal Hernia with GastricPerforation : A Case Report
- Laparoscopic total extraperitoneal repair for incarcerated inguinal hernia
