Adjustable Ghajar Guide Technique for Accurate Placement of Ventricular Catheters: A Pilot Study
- Affiliations
-
- 1Department of Neurosurgery and Research Center for Neurosurgical Robotic Systems, Kyungpook National University School of Medicine, Daegu, Korea. jparkmd@hotmail.com
- KMID: 2457969
- DOI: http://doi.org/10.3340/jkns.2016.1011.004
Abstract
OBJECTIVE
An adjustable Ghajar guide is presented to improve the accuracy of the original Ghajar guide technique. The accuracy of the adjustable Ghajar guide technique is also investigated.
METHODS
The coronal adjustment angle from the orthogonal catheter trajectory at Kocher's point is determined based on coronal head images using an electronic picture archiving and communication system. For the adjustable Ghajar guide, a protractor is mounted on a C-shaped basal plate that is placed in contact with the margin of a burrhole, keeping the central 0° line of the protractor orthogonal to the calvarial surface. A catheter guide, which is moved along the protractor and fixed at the pre-determined adjustment angle, is then used to guide the ventricular catheter into the frontal horn adjacent to the foramen of Monro. The adjustable Ghajar guide technique was applied to 20 patients, while a freehand technique based on the surface anatomy of the head was applied to another 47 patients. The accuracy of the ventricular catheter placement was then evaluated using postoperative computed tomography scans.
RESULTS
For the adjustable Ghajar guide technique (AGT) patients, the bicaudate index ranged from 0.23 to 0.33 (mean±standard deviation [SD]: 0.27±0.03) and the adjustment angle ranged from 0° to 10° (mean±SD: 5.2°±3.2°). All the AGT patients experienced successful cerebrospinal fluid diversion with only one pass of the catheter. Optimal placement of the ventricular catheter in the ipsilateral frontal horn approximating the foramen of Monro (grade 1) was achieved in 19 patients (95.0%), while a suboptimal trajectory into a lateral corner of the frontal horn passing along a lateral wall of the frontal horn (grade 3) occurred in 1 patient (5.0%). Thus, the AGT patients experienced a significantly higher incidence of optimal catheter placement than the freehand catheterized patients (95.0% vs. 68.3%, p=0.024). Moreover, none of the AGT patients experienced any tract hemorrhages along the catheter or procedure-related complications.
CONCLUSION
The proposed adjustable Ghajar guide technique, using angular adjustment in the coronal plane from the orthogonal trajectory at Kocher's point, facilitates accurate freehand placement of a ventricular catheter for hydrocephalic patients.
MeSH Terms
Figure
-
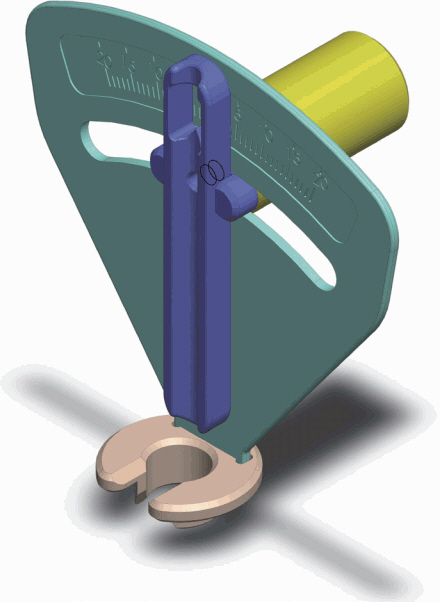
Fig. 1 Illustration of the adjustable Ghajar guide.

Fig. 2 Coronal computed tomography images showing the radiographic simulation of the catheter trajectories to determine the adjustment angle for the adjustable Ghajar guide technique. A: A burrhole site (arrow) is marked at a point 3 cm lateral to the midline of the skull. B: An approximately 3 cm-long chord (red line) is drawn with both ends equidistant from the burrhole site on the circular line outlining the calvarial surface. C: A perpendicular line starting at the middle of the chord is drawn to the ventricular system. D: The ideal catheter trajectory toward the foramen of Monro is drawn from the middle of the chord. The adjustment angle, the difference between the catheter trajectory (90°) perpendicular to the calvarial surface and the ideal catheter trajectory (95°), is 5°.
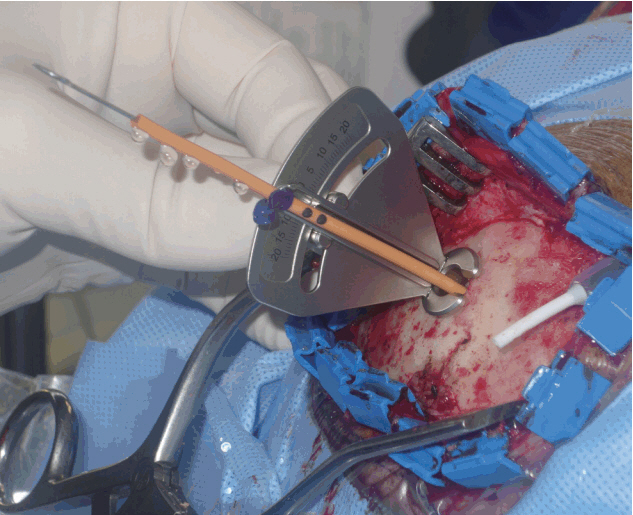
Fig 3 Intraoperative photograph showing the adjustable Ghajar guide used for the ventriculoperitoneal shunt.
Reference
-
References
1. Abu-Serieh B, Ghassempour K, Duprez T, Raftopoulos C. Stereotactic ventriculoperitoneal shunting for refractory idiopathic intracranial hypertension. Neurosurgery. 60:1039–1043. discussion 1043–1044. 2007.
Article2. Ann JM, Bae HG, Oh JS, Yoon SM. Device for catheter placement of external ventricular drain. J Korean Neurosurg Soc. 59:322–324. 2016.
Article3. Azeem SS, Origitano TC. Ventricular catheter placement with a frameless neuronavigational system: a 1-year experience. Neurosurgery. 60(4 Suppl 2):243–247. discussion 247–248. 2007.4. Bergsneider M, Stiner E. Management of adult hydrocephalus: Shunting. Winn HR, editor. Youmans Neurological Surgery. ed 6. Philadelphia: Saunders;2011. 1:p. 515–524.5. Clark S, Sangra M, Hayhurst C, Kandasamy J, Jenkinson M, Lee M, et al. The use of noninvasive electromagnetic neuronavigation for slit ventricle syndrome and complex hydrocephalus in a pediatric population. J Neurosurg Pediatr. 2:430–434. 2008.
Article6. Epstein MH, Duncan JA. Surgical management of hydrocephalus in adults. Schmidek HH, editor. Schmidek & Sweet Operative Neurosurgical Techniques: Indications, Methods, and Results. ed 4. Philadelphia: Saunders;2000. 1:p. 595–603.7. Ghajar JB. A guide for ventricular catheter placement. Technical note J Neurosurg. 63:985–986. 1985.
Article8. Gil Z, Siomin V, Beni-Adani L, Sira B, Constantini S. Ventricular catheter placement in children with hydrocephalus and small ventricles: the use of a frameless neuronavigation system. Childs Nerv Syst. 18:26–29. 2002.
Article9. Huyette DR, Turnbow BJ, Kaufman C, Vaslow DF, Whiting BB, Oh MY. Accuracy of the freehand pass technique for ventriculostomy catheter placement: retrospective assessment using computed tomography scans. J Neurosurg. 108:88–91. 2008.
Article10. Jung N, Kim D. Effect of electromagnetic navigated ventriculoperitoneal shunt placement on failure rates. J Korean Neurosurg Soc. 53:150–154. 2013.
Article11. Kandasamy J, Hayhurst C, Clark S, Jenkinson MD, Byrne P, Karabatsou K, et al. Electromagnetic stereotactic ventriculoperitoneal csf shunting for idiopathic intracranial hypertension: a successful step forward? World Neurosurg. 75:155–160. discussion 32–33. 2011.
Article12. Lind CR, Correia JA, Law AJ, Kejriwal R. A survey of surgical techniques for catheterising the cerebral lateral ventricles. J Clin Neurosci. 15:886–890. 2008.
Article13. Moran D, Kosztowski TA, Jusué-Torres I, Orkoulas-Razis D, Ward A, Carson K, et al. Does CT wand guidance improve shunt placement in patients with hydrocephalus? Clin Neurol Neurosurg. 132:26–30. 2015.
Article14. O’Leary ST, Kole MK, Hoover DA, Hysell SE, Thomas A, Shaffrey CI. Efficacy of the Ghajar Guide revisited: a prospective study. J Neurosurg. 92:801–803. 2000.
Article15. Park J, Son W, Park KS, Kim MY, Lee J. Calvarial slope affecting accuracy of Ghajar Guide technique for ventricular catheter placement. J Neurosurg. 124:1429–1433. 2016.
Article16. Piatt JH. Hydrocephalus: Treatment. Wilkins RH, Rengachary SS, editors. Neurosurgery. ed 2. New York: McGraw-Hill;1996. 3:p. 3633–3643.17. Ravindra VM, Kraus KL, Riva-Cambrin JK, Kestle JR. The need for cost-effective neurosurgical innovation--a global surgery initiative. World Neurosurg. 84:1458–1461. 2015.
Article18. Rehman T, Rehman Au, Ali R, Rehman A, Bashir H, Ahmed Bhimani S, et al. A radiographic analysis of ventricular trajectories. World Neurosurg. 80:173–178. 2013.
Article19. Rehman T, Rehman AU, Rehman A, Bashir HH, Ali R, Bhimani SA, et al. A US-based survey on ventriculostomy practices. Clin Neurol Neurosurg. 114:651–654. 2012.
Article20. Schaumann A, Thomale UW. Guided application of ventricular catheters (GAVCA)--multicentre study to compare the ventricular catheter position after use of a catheter guide versus freehand application: study protocol for a randomised trail. Trials. 14:428. 2013.
Article21. Thomale UW, Knitter T, Schaumann A, Ahmadi SA, Ziegler P, Schulz M, et al. Smartphone-assisted guide for the placement of ventricular catheters. Childs Nerv Syst. 29:131–139. 2013.
Article22. Wilson TJ, Stetler WR Jr, Al-Holou WN, Sullivan SE. Comparison of the accuracy of ventricular catheter placement using freehand placement, ultrasonic guidance, and stereotactic neuronavigation. J Neurosurg. 119:66–70. 2013.
Article23. Woerdeman PA, Willems PW, Han KS, Hanlo PW, Berkelbach van der Sprenkel JW. Frameless stereotactic placement of ventriculoperitoneal shunts in undersized ventricles: a simple modification to free-hand procedures. Br J Neurosurg. 19:484–487. 2005.
Article24. Woo H, Kang DH, Park J. Preoperative determination of ventriculostomy trajectory in ventriculoperitoneal shunt surgery using a simple modification of the standard coronal MRI. J Clin Neurosci. 20:1754–1758. 2013.
Article25. Yamada SM, Yamada S, Goto Y, Nakaguchi H, Murakami M, Hoya K, et al. A simple and consistent technique for ventricular catheter insertion using a tripod. Clin Neurol Neurosurg. 114:622–666. 2012.
Article26. Yim B, Reid Gooch M, Dalfino JC, Adamo MA, Kenning TJ. Optimizing ventriculoperitoneal shunt placement in the treatment of idiopathic intracranial hypertension: an analysis of neuroendoscopy, frameless stereotaxy, and intraoperative CT. Neurosurg Focus. 40:E12. 2016.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Accurate Placement of Parieto-occipital Ventricular Catheter Using CT Parameters
- The Accuracy of Implant Placement According to the Height of the Surgical Guide Hole
- Band Slippage after Laparoscopic Adjustable Gastric Banding (LAGB)
- Percutaneous Catheter Drainage of Thoracic Fluid: The Usefulness and Safety of Bedside Trocar Placement under Ultrasound Guidance
- Safe Placement of Urethral Foley Catheter Using Guide Wire in Patient with False Passage
