Intradural Transpetrosectomy for Petrous Apex Meningiomas
- Affiliations
-
- 1Department of Neurosurgery, Renji Hospital, Shanghai JiaoTong University School of Medicine, Shanghai, China. handongh9999@163.com
- 2Department of Neurosurgery, Pudong Hospital, Shanghai FuDan University School of Medicine, Shanghai, China.
- KMID: 2457952
- DOI: http://doi.org/10.3340/jkns.2018.0015
Abstract
OBJECTIVE
This study aimed to assess the surgical results of the intradural transpetrosectomy for petrous apex meningiomas (PAMs). In addition, we describe the methods and techniques used to expose and manage superior petrous vein and greater superficial petrosal nerve.
METHODS
The authors conducted a retrospective study of 16 patients with PAMs operated by the senior author via the intradural transpetrosectomy between February 2012 to May 2017. We reviewed patient data regarding the general characteristics, surgical technique and surgery-related outcomes and adopted a combined follow-up strategy of clinic and telephone contacts to evaluate postoperative complications.
RESULTS
Simpson grade I and II resection was performed in 10 out of 16 cases (62.5%), and grade III resection were reported in the remaining six cases (37.5%) with no resultant mortality. The mean Karnofsky Performance Status score was 85.6 preoperatively and improved to 91.9 postoperatively, with a mean follow-up period of 34.4 months (range, 6-66 months). Tumor recurrence was found in two patients and they underwent the second surgical operation.
CONCLUSION
PAMs could be completely resected by the intradural transpetrosectomy with an improved survival rate and postoperative life quality. Superior petrous vein and greater superficial petrosal nerve should be managed properly in avoidance of postoperative complications. Finally, most meningioma inside cavernous sinus or adhered to brainstem could be totally removed without postoperative complications.
Keyword
MeSH Terms
Figure
-
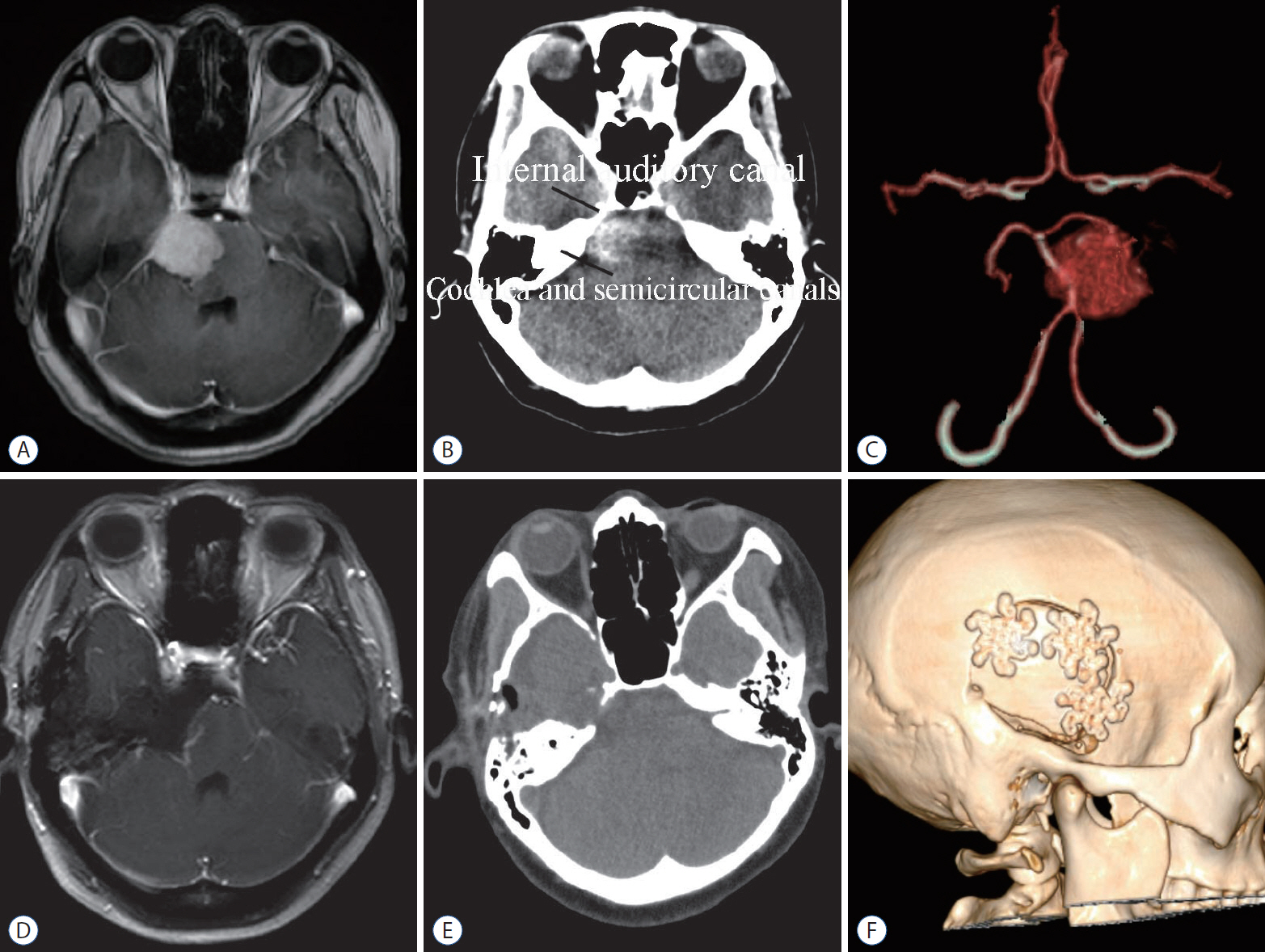
Fig. 1. A : Preoperative MRI, axial view : an enhanced petrous apex meningioma was seen around the right Meckel’s cave and extend into the supratentorial region. B : Preoperative CT : relationship between bone and tumor. C : Preoperative 3D-CT angiography : right posterior cerebral artery was compressed and replaced superior to the tumor. D : Postoperative MRI : no residual tumor. E : Postoperative CT : the drilling extent of petrous bone. F : Postoperative 3D-CT reconstruction : bone flap was placed back. MRI : magnetic resonance imaging, CT : computed tomography.

Fig. 2. A : Patient’s position and skin incision. B : The size of bone flap. C : Superior petrosal sinus groove was clipped with titanium clips. D : Identified the internal auditory canal by Garcia-Ibanz method [5]. E : Drilling extent. ① 1.5 cm : from the trigeminal nerve pressure trace to the internal auditory canal; ② 1.0 cm : from the petrous edge to the petrous section of internal carotid artery; ③ 1.0 cm : from the petrous tip to the petrosal sinus. F : Separated neurovascular structures from tumor. FS : foramen spinosum, GSPN : greater superficial petrosal nerve, AE : arcuate eminence, IAC : internal auditory canal, Gr. : great, For. : foramen, Trig. : trigminal, Pet. : petrosal, N. : nerve, Occip. : occipital, Arc. : arcuate, Emin. : eminece, Int. : internal, Ac. : arcuate, Sig. : sigmoid.
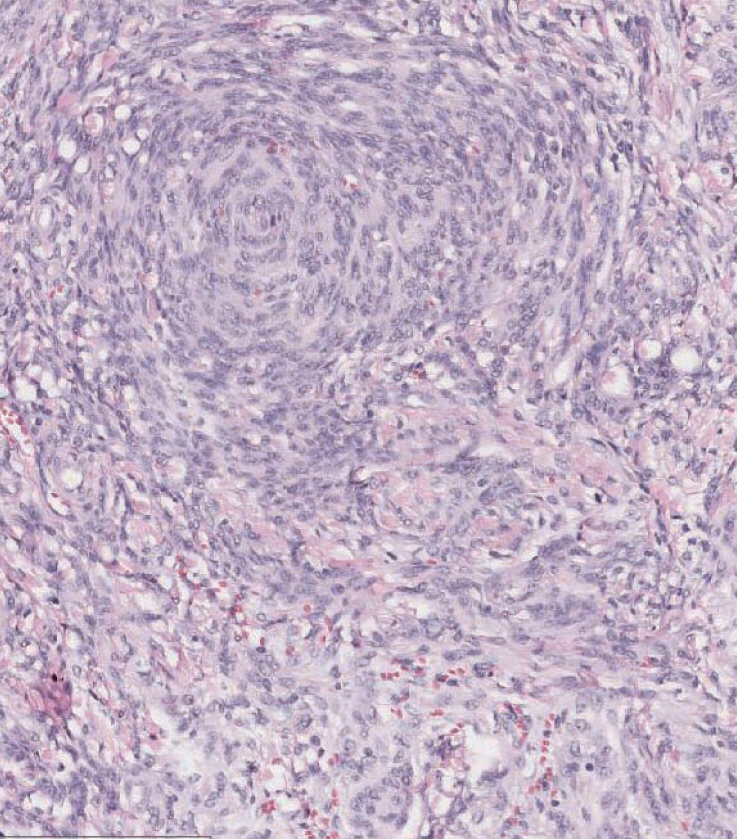
Fig. 3. Histological examination of meningioma following hematoxylin and eosin staining (×200).
Reference
-
References
1. Altieri R, Sameshima T, Pacca P, Crobeddu E, Garbossa D, Ducati A, et al. Detailed anatomy knowledge: first step to approach petroclival meningiomas through the petrous apex. Anatomy lab experience and surgical series. Neurosurg Rev. 40:231–239. 2017.
Article2. Bochenek Z, Kukwa A. An extended approach through the middle cranial fossa to the internal auditory meatus and the cerebello-pontine angle. Acta Otolaryngol. 80:410–414. 1975.
Article3. Borghei-Razavi H, Tomio R, Fereshtehnejad SM, Shibao S, Schick U, Toda M, et al. Anterior petrosal approach: The safety of Kawase triangle as an anatomical landmark for anterior petrosectomy in petroclival meningiomas. Clin Neurol Neurosurg. 139:282–287. 2015.
Article4. Cui H, Zhou CF, Bao YH, Wang MS, Wang Y. Extended suboccipital retrosigmoid surgical approach is effective for resection of petrous apex meningioma. J Craniofac Surg. 27:e429–e433. 2016.
Article5. Garcia-Ibanez E, Garcia-Ibanez JL. Middle fossa vestibular neurectomy: a report of 373 cases. Otolaryngol Head Neck Surg. 88:486–490. 1980.
Article6. Ichimura S, Hori S, Hecht N, Czabanka M, Vajkoczy P. Intradural anterior transpetrosal approach. Neurosurg Rev. 39:625–631. 2016.
Article7. Janjua MB, Caruso JP, Greenfield JP, Souweidane MM, Schwartz TH. The combined transpetrosal approach: Anatomic study and literature review. J Clin Neurosci. 41:36–40. 2017.
Article8. Jittapiromsak P, Sabuncuoglu H, Deshmukh P, Nakaji P, Spetzler RF, Preul MC. Greater superficial petrosal nerve dissection: back to front or front to back? Neurosurgery. 64(5 Suppl 2):253–258. discussion 258-259. 2009.
Article9. Kawase T, Shiobara R, Toya S. Anterior transpetrosal-transtentorial approach for sphenopetroclival meningiomas: surgical method and results in 10 patients. Neurosurgery. 28:869–875. discussion 875-876. 1991.
Article10. Lee HS, Kim JH, Lee JI. Glioblastoma following radiosurgery for meningioma. J Korean Neurosurg Soc. 51:98–101. 2012.
Article11. Lee SR, Yang KA, Kim SK, Kim SH. Radiation-induced intratumoral necrosis and peritumoral edema after gamma knife radiosurgery for intracranial meningiomas. J Korean Neurosurg Soc. 52:98–102. 2012.
Article12. Li D, Tang J, Ren C, Wu Z, Zhang LW, Zhang JT. Surgical management of medium and large petroclival meningiomas: a single institution’s experience of 199 cases with long-term follow-up. Acta neurochir (Wien). 158:409–425. discussion 425. 2016.
Article13. Matsushima T, Kawashima M, Inoue K, Matsushima K. Anatomy of the superior petrosal veins and their exposure and management during petrous apex meningioma surgery using the lateral suboccipital retrosigmoid approach. Neurosurg Rev. 37:535–456. 2014.
Article14. Maurer AJ, Safavi-Abbasi S, Cheema AA, Glenn CA, Sughrue ME. Management of petroclival meningiomas: a review of the development of current therapy. J Neurol Surg B Skull Base. 75:358–367. 2014.
Article15. Miller ME, Mastrodimos B, Cueva RA. Facial nerve function after the extended translabyrinthine approach. J Neurol Surg B Skull Base. 76:1–6. 2015.
Article16. Morisako H, Goto T, Ohata K. Petroclival meningiomas resected via a combined transpetrosal approach: surgical outcomes in 60 cases and a new scoring system for clinical evaluation. J Neurosurg. 122:373–380. 2015.
Article17. Oh IH, Park BJ, Choi SK, Lim YJ. Transient neurologic deterioration after total removal of parasagittal meningioma including completely occluding superior sagittal sinus. J Korean Neurosurg Soc. 46:71–73. 2009.
Article18. Ohata K, Haque M, Morino M, Nagai K, Nishio A, Nishijima Y, et al. Occlusion of the sigmoid sinus after surgery via the presigmoidal-transpetrosal approach. J Neurosurg. 89:575–584. 1998.
Article19. Samii M, Ammirati M, Mahran A, Bini W, Sepehrnia A. Surgery of petroclival meningiomas: report of 24 cases. Neurosurgery. 24:12–17. 1989.
Article20. Sharma M, Ambekar S, Guthikonda B, Nanda A. A Comparison between the Kawase and extended retrosigmoid approaches (Retrosigmoid transtentorial and retrosigmoid intradural suprameatal approaches) for accessing the petroclival tumors. A cadaveric study. J Neurol Surg B Skull Base. 75:171–176. 2014.
Article21. Shibao S, Borghei-Razavi H, Orii M, Yoshida K. Anterior transpetrosal approach combined with partial posterior petrosectomy for petroclival meningiomas with posterior extension. World neurosurg. 84:574–579. 2015.
Article22. Tripathi M, Deo RC, Suri A, Srivastav V, Baby B, Kumar S, et al. Quantitative analysis of the Kawase versus the modified Dolenc-Kawase approach for middle cranial fossa lesions with variable anteroposterior extension. J Neurosurg. 123:14–22. 2015.
Article23. Tummala RP, Coscarella E, Morcos JJ. Transpetrosal approaches to the posterior fossa. Neurosurg Focus. 19:E6. 2005.
Article24. Xiao X, Zhang L, Wu Z, Zhang J, Jia G, Tang J, et al. Surgical resection of large and giant petroclival meningiomas via a modified anterior transpetrous approach. Neurosurg Rev. 36:587–593. discussion 593-594. 2013.
Article25. Youssef S, Kim EY, Aziz KM, Hemida S, Keller JT, van Loveren HR. The subtemporal interdural approach to dumbbell-shaped trigeminal schwannomas: cadaveric prosection. Neurosurgery. 59(4 Suppl 2):ONS270–ONS277. 2006.
Article26. Zhong J, Li ST, Xu SQ, Wan L, Wang X. Management of petrosal veins during microvascular decompression for trigeminal neuralgia. Neurol Res. 30:697–700. 2008.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical Anatomy for the Infracochlear Approach to the Petrous Apex
- Petrous Apex Cephalocele: Report of Two Cases and Review of the Literature
- Petrous Apex Pneumatization on Computed Tomography
- Surgical Anatomical Landmarks for Petrous Apex
- A Case of Huge Congenital Cholesteatoma of Petrous Apex Treated With Translabyrinthine Marsupialization
