Intervention for Urologic Trauma
- Affiliations
-
- 1Department of Radiology, Pusan National University Hospital, Busan, Korea. changho.jeon@gmail.com
- 2Medical Research Institute, Pusan National University Hospital, Busan, Korea.
- KMID: 2457446
- DOI: http://doi.org/10.3348/jksr.2019.80.4.667
Abstract
- Urinary tract injuries occur in up to 10% of patients with abdominal trauma, and the kidney is the most commonly injured structure of the urinary system. The kidney is the third most common abdominal organ to be injured by trauma, following the spleen and liver, in that order. The American Association for the Surgery of Trauma kidney injury scale is the most commonly used classification system for blunt renal injuries, which grades renal injury based on the size of laceration and its proximity to the renal hilum on CT. CT aids in delineating the most important features of urological injury that affect the diagnosis and management, including interventions. The major renal injuries are usually surgical emergencies. The current trend toward a more conservative management of renal trauma and advances in interventional radiology in the field of trauma may increase the use of interventional procedures for patients with renal injury. Urethral injuries can be anterior or posterior depending on the injury site, and interventional urethral realignment plays an important role in the treatment of urethral injury and surgical repair or endoscopic urethral realignment. Therefore, in this paper, we provide a literature review and discuss the efficacy and clinical significance of intervention for urologic trauma.
MeSH Terms
Figure
-

Fig. 1 A 57-year-old man showing a shattered kidney (The American Association for Surgery of Trauma V) after slipping. A. CT scan shows a shattered kidney presenting as renal parenchyma completely separated from the renal capsule and contrast extravasation. B. Left renal angiography confirms a shattered kidney. In addition, contrast leakage and pseudoaneurysm are demonstrated. C. Selective embolization for the two feeders of contrast leakage and pseudoaneurysm using a mixture with 1:3 ratio of N-butyl-2-cyanoacrylate to lipiodol. D. Follow-up CT after 2 months shows no perirenal fluid collection or urine leakage. The degree of enhancement is mildly reduced, but the remodeled kidney shows better renal perfusion on the coronal image.
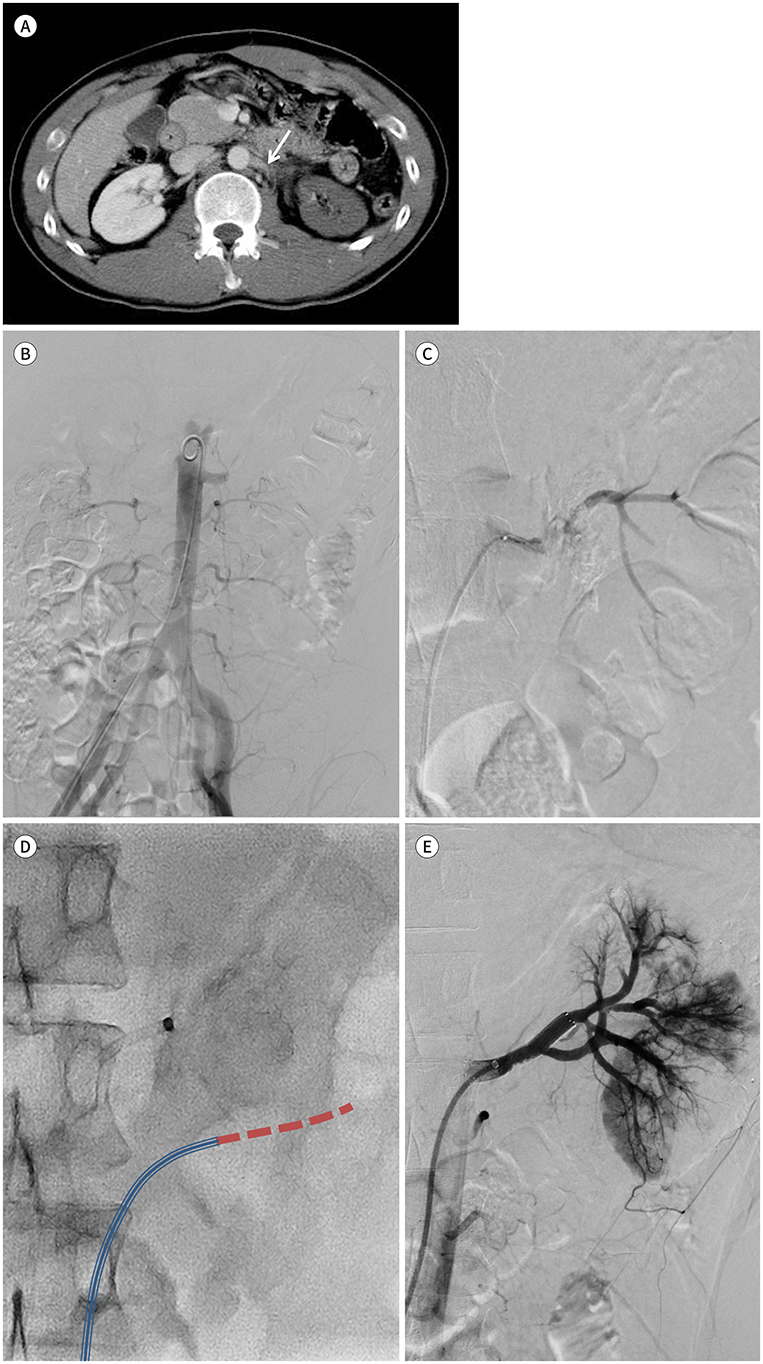
Fig. 2 27-year-old man with main renal artery injury struck by an industrial robot. A. CT scan shows discontinuation of the left renal artery (arrow) and almost no enhancement in the left kidney. B. The left kidney is not visible on suprarenal abdominal aortography probably due to the transection or flow-limiting dissection of the left main renal artery. C. The distal flow is faintly visible when contrast was injected through the 5-Fr catheter. However, the 0.035-inch hydrophilic coated guidewire could not pass beyond this point because of the acute vessel angle. D. After changing the vessel angle using the 6-Fr angled guiding sheath (blue triple line), we succeeded in administering the 0.035-inch hydrophilic coated guidewire (red dotted line) up to the distal portion. E. After the deployment of the 8-mm self-expandable metallic stent, completion renal angiography shows restoration of the parenchymal perfusion and venous drainage.
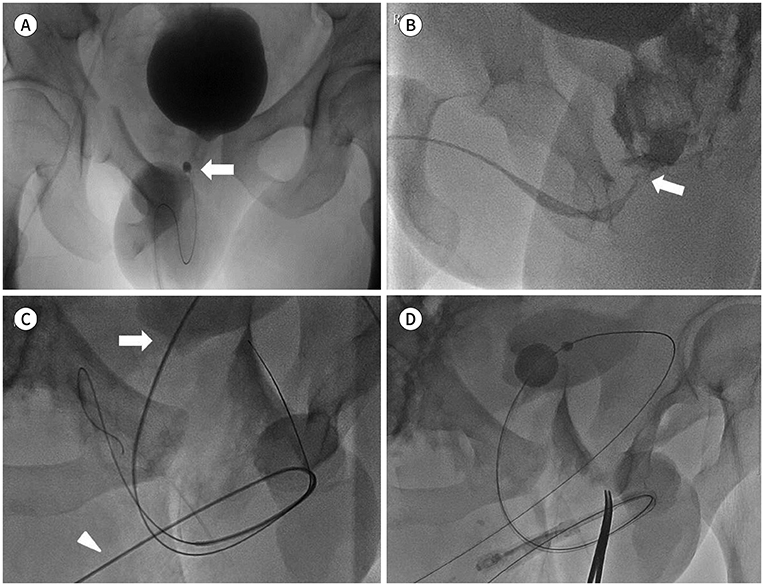
Fig. 3 Interventional realignment for posterior urethral disruption. A 32-year-old man with posterior urethral disruption after a motocycle accident. A. Fluoroscopy reveals a complex pelvic fracture with contrast filling of the urinary bladder. The end (arrow) of the Foley catheter is not in the bladder. B. Retrograde urethrogram shows posterior urethral disruption. The end of the disrupted membranous urethra has a beak appearance (arrow). C. Supported by the 5-Fr catheter, a 0.035-inch hydrophilic coated guidewire (arrowhead) was located in the free space in the pelvic cavity without detecting the disrupted contralateral proximal urethra (retrograde approach). Another 0.035-inch hydrophilic coated guidewire (arrow), which was loaded in the 5-Fr catheter, was passed through the suprapubic cystostomy and navigated to pass through the site of the posterior urethral disruption so as to reach the external urethral orifice (antegrade approach). D. A 16-Fr Foley catheter was inserted in the bladder over the guidewire (through-and-through technique) for posterior urethral realignment.
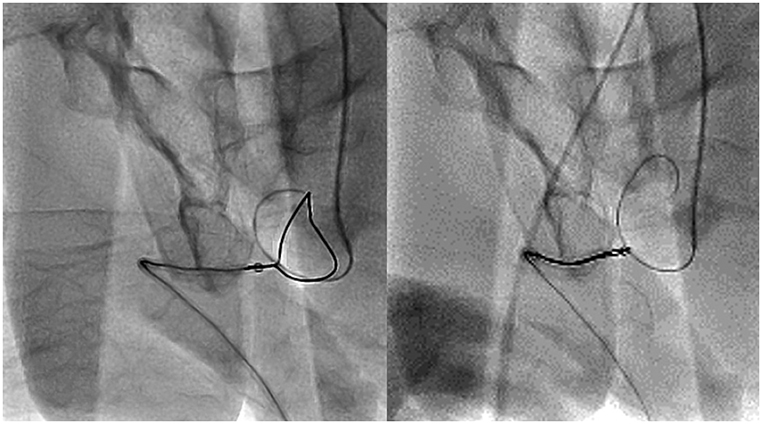
Fig. 4 Snare catheter being used for effectively grasping the guidewire with the retrograde approach.
Reference
-
1. Herschorn S, Radomski SB, Shoskes DA, Mahoney J, Hirshberg E, Klotz L. Evaluation and treatment of blunt renal trauma. J Urol. 1991; 146:274–276.2. Wessells H, Suh D, Porter JR, Rivara F, MacKenzie EJ, Jurkovich GJ, et al. Renal injury and operative management in the United States: results of a population-based study. J Trauma. 2003; 54:423–430.3. Wessells H, McAninch JW, Meyer A, Bruce J. Criteria for nonoperative treatment of significant penetrating renal lacerations. J Urol. 1997; 157:24–27.4. Lee MS, Kim SH, Kim BS, Choi GM, Huh JS. The efficacy of primary interventional urethral realignment for the treatment of traumatic urethral injuries. J Vasc Interv Radiol. 2016; 27:226–231.5. Patel P, Duttaroy D, Kacheriwala S. Management of renal injuries in blunt abdominal trauma. J Res Med Dent Sci. 2014; 2:38–42.6. Sangthong B, Demetriades D, Martin M, Salim A, Brown C, Inaba K, et al. Management and hospital outcomes of blunt renal artery injuries: analysis of 517 patients from the National Trauma Data Bank. J Am Coll Surg. 2006; 203:612–617.7. Carroll PR, McAninch JW, Klosterman P, Greenblatt M. Renovascular trauma: risk assessment, surgical management, and outcome. J Trauma. 1990; 30:547–552.8. Cass AS, Bubrick M, Luxenberg M, Gleich P, Smith C. Renal pedicle injury in patients with multiple injuries. J Trauma. 1985; 25:892–896.9. Plainfosse MC, Calonge VM, Beyloune-Mainardi C, Glotz D, Duboust A. Vascular complications in the adult kidney transplant recipient. J Clin Ultrasound. 1992; 20:517–527.10. Cass AS, Vieira J. Comparison of IVP and CT findings in patients with suspected severe renal injury. Urology. 1987; 29:484–487.11. McGahan JP, Richards JR, Jones CD, Gerscovich EO. Use of ultrasonography in the patient with acute renal trauma. J Ultrasound Med. 1999; 18:207–213.12. Perry MJ, Porte ME, Urwin GH. Limitations of ultrasound evaluation in acute closed renal trauma. J R Coll Surg Edinb. 1997; 42:420–422.13. Bretan PN Jr, McAninch JW, Federle MP, Jeffrey RB Jr. Computerized tomographic staging of renal trauma: 85 consecutive cases. J Urol. 1986; 136:561–565.14. McAninch JW, Federle MP. Evaluation of renal injuries with computerized tomography. J Urol. 1982; 128:456–460.15. Alonso RC, Nacenta SB, Martinez PD, Guerrero AS, Fuentes CG. Kidney in danger: CT findings of blunt and penetrating renal trauma. Radiographics. 2009; 29:2033–2053.16. Goldman SM, Sandler CM. Urogenital trauma: imaging upper GU trauma. Eur J Radiol. 2004; 50:84–95.17. Carpio F, Morey AF. Radiographic staging of renal injuries. World J Urol. 1999; 17:66–70.18. Wright JL, Nathens AB, Rivara FP, Wessells H. Renal and extrarenal predictors of nephrectomy from the national trauma data bank. J Urol. 2006; 175:970–975.19. Armenakas NA, Duckett CP, McAninch JW. Indications for nonoperative management of renal stab wounds. J Urol. 1999; 161:768–771.20. Broghammer JA, Fisher MB, Santucci RA. Conservative management of renal trauma: a review. Urology. 2007; 70:623–629.21. Matthews LA, Smith EM, Spirnak JP. Nonoperative treatment of major blunt renal lacerations with urinary extravasation. J Urol. 1997; 157:2056–2058.22. Santucci RA, McAninch JW, Safir M, Mario LA, Service S, Segal MR. Validation of the American Association for the surgery of trauma organ injury severity scale for the kidney. J Trauma. 2001; 50:195–200.23. Brewer ME Jr, Strnad BT, Daley BJ, Currier RP, Klein FA, Mobley JD, et al. Percutaneous embolization for the management of grade 5 renal trauma in hemodynamically unstable patients: initial experience. J Urol. 2009; 181:1737–1741.24. Stewart AF, Brewer ME Jr, Daley BJ, Klein FA, Kim ED. Intermediate-term follow-up of patients treated with percutaneous embolization for grade 5 blunt renal trauma. J Trauma. 2010; 69:468–470.25. Bruce LM, Croce MA, Santaniello JM, Miller PR, Lyden SP, Fabian TC. Blunt renal artery injury: Incidence, diagnosis, and management. Am Surg. 2001; 67:550–554.26. Brown MF, Graham JM, Mattox KL, Feliciano DV, DeBakey ME. Renovascular trauma. Am J Surg. 1980; 140:802–805.27. Knudson MM, Harrison PB, Hoyt DB, Shatz DV, Zietlow SP, Bergstein JM, et al. Outcome after major renovascular injuries: a Western trauma association multicenter report. J Trauma. 2000; 49:1116–1122.28. McGuire J, Bultitude MF, Davis P, Koukounaras J, Royce PL, Corcoran NM. Predictors of outcome for blunt high grade renal injury treated with conservative intent. J Urol. 2011; 185:187–191.29. Beaujeux R, Saussine C, Al-Fakir A, Boudjema K, Roy C, Jacqmin D, et al. Superselective endo-vascular treatment of renal vascular lesions. J Urol. 1995; 153:14–17.30. Matsumoto J, Lohman BD, Morimoto K, Ichinose Y, Hattori T, Taira Y. Damage control interventional radiology (DCIR) in prompt and rapid endovascular strategies in trauma occasions (PRESTO): a new paradigm. Diagn Interv Imaging. 2015; 96:687–691.31. Howell GM, Peitzman AB, Nirula R, Rosengart MR, Alarcon LH, Billiar TR, et al. Delay to therapeutic interventional radiology postinjury: time is of the essence. J Trauma. 2010; 68:1296–1300.32. Pryor JP, Braslow B, Reilly PM, Gullamondegi O, Hedrick JH, Schwab CW. The evolving role of interventional radiology in trauma care. J Trauma. 2005; 59:102–104.33. Fisher RG, Ben-Menachem Y, Whigham C. Stab wounds of the renal artery branches: angiographic diagnosis and treatment by embolization. AJR Am J Roentgenol. 1989; 152:1231–1235.34. Whigham CJ Jr, Bodenhamer JR, Miller JK. Use of the Palmaz stent in primary treatment of renal artery intimal injury secondary to blunt trauma. J Vasc Interv Radiol. 1995; 6:175–178.35. Bookstein JJ, Goldstein HM. Successful management of postbiopsy arteriovenous fistula with selective arterial embolization. Radiology. 1973; 109:535–536.36. Santucci RA, McAninch JW. Diagnosis and management of renal trauma: past, present, and future. J Am Coll Surg. 2000; 191:443–451.37. May AM, Darwish O, Dang B, Monda JJ, Adsul P, Syed J, et al. Successful nonoperative management of highgrade blunt renal injuries. Adv Urol. 2016; 2016:3568076.38. Hagiwara A, Sakaki S, Goto H, Takenega K, Fukushima H, Matuda H, et al. The role of interventional radiology in the management of blunt renal injury: a practical protocol. J Trauma. 2001; 51:526–531.39. Goodman DN, Saibil EA, Kodama RT. Traumatic intimal tear of the renal artery treated by insertion of a Palmaz stent. Cardiovasc Intervent Radiol. 1998; 21:69–72.40. Paul JL, Otal P, Perreault P, Galinier P, Baunin C, Puget C, et al. Treatment of posttraumatic dissection of the renal artery with endoprosthesis in a 15-year-old girl. J Trauma. 1999; 47:169–172.41. Villas PA, Cohen G, Putnam SG 3rd, Goldberg A, Ball D. Wallstent placement in a renal artery after blunt abdominal trauma. J Trauma. 1999; 46:1137–1139.42. Lopera JE, Suri R, Kroma G, Gadani S, Dolmatch B. Traumatic occlusion and dissection of the main renal artery: endovascular treatment. J Vasc Interv Radiol. 2011; 22:1570–1574.43. Cohen JK, Berg G, Carl GH, Diamond DD. Primary endoscopic realignment following posterior urethral disruption. J Urol. 1991; 146:1548–1550.44. Melekos MD, Pantazakos A, Daouaher H, Papatsoris G. Primary endourologic re-establishment of urethal continuity after disruption of prostatomembranous urethra. Urology. 1992; 39:135–138.45. Moudouni SM, Patard JJ, Manunta A, Guiraud P, Lobel B, Guillé F. Early endoscopic realignment of posttraumatic posterior urethral disruption. Urology. 2001; 57:628–632.46. Clark WR, Patterson DE, Williams HJ Jr. Primary radiologic realignment of membranous urethral disruptions. Urology. 1992; 39:182–184.47. Londergan TA, Gundersen LH, Van Every MJ. Early fluoroscopic realignment for traumatic urethral injuries. Urology. 1997; 49:101–103.48. Kozar RA, Crandall M, Shanmuganathan K, Zarzaur BL, Coburn M, Cribari C, et al. Organ injury scaling 2018 update: spleen, liver, and kidney. J Trauma Acute Care Surg. 2018; 85:1119–1122.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Role of Transarterial Embolization in the Management of Urologic Diseases
- The Clinical Characteristics of Urologic Patients Who Visited Emergency Center
- The incidence of urologic complications requiring urologic procedure in radical hysterectomy and difference between abdominal radical hysterectomy and laparoscopic radical hysterectomy
- Trauma and Reconstruction of the External Genitalia
- Anesthetic considerations for urologic surgeries
