Can we delineate preoperatively the right and ventral margins of caudate lobe of the liver?
- Affiliations
-
- 1Division of Liver Transplantation and Hepatobiliary Surgery, Department of Surgery, Ajou University School of Medicine, Suwon, Korea. wanghj@ajou.ac.kr
- 2Department of Hepatobiliary Surgery, Jiangxi Cancer Hospital, Jiangxi, China.
- KMID: 2455972
- DOI: http://doi.org/10.4174/astr.2019.97.3.124
Abstract
- PURPOSE
Complete removal of the caudate lobe, which is sometimes necessary, is accomplished via isolated caudate lobectomy or hepatectomy that includes the caudate lobe. It is impossible, however, to confirm the right and ventral margins of the caudate lobe by preoperative imaging. This study was undertaken to determine whether we could identify the right and ventral margins of the caudate lobe preoperatively using Synapse 3D visualization software.
METHODS
Ninety-four preoperative 3-dimensional (3D) computed tomographic images (1-mm slices) of the liver from candidate donors were examined. The images of the caudate lobe were subjected to a counter-staining method according to Synapse 3D to delineate their dimensions. We first examined whether the right margin of the caudate lobe exceeded the plane formed by the root of the right hepatic vein (RHV) and the right side of the inferior vena cava (IVC). Second, we determined whether the ventral margin of the caudate lobe exceeded the plane formed by the root of the middle hepatic vein (MHV) and the root of the RHV.
RESULTS
For the right margin, 17 cases (18%) exceeded the RHV-IVC plane by a mean of 10.2 mm (range, 2.4-27.2 mm). For the ventral margin, 28 cases (30%) exceeded the MHV-RHV plane by a mean of 17.4 mm (range, 1.2-49.1 mm).
CONCLUSION
Evaluating the anatomy of caudate lobe using Synapse 3D preoperatively could be helpful for more precise anatomical resection of the caudate lobe.
MeSH Terms
Figure
-
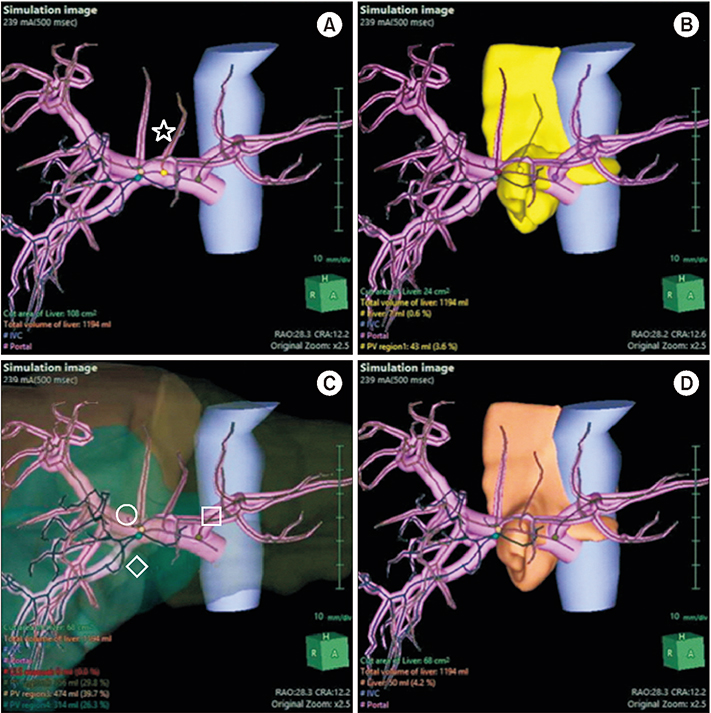
Fig. 1 The caudate parenchyma was delineated using a counter-staining technique. Hepatic veins, hepatic arteries, and bile ducts are hidden to identify images more easily. (A) By hiding the hepatic parenchyma, the portal vein branch of the paracaval portion can be seen (star). (B) By clicking on the portal vein branch of the paracaval portion, the parenchyma of caudate lobe is shown (yellow). (C) In the same case, we clicked on the left portal vein (square), right anterior portal vein (circle), and right posterior portal vein (diamond), respectively, which then showed the corresponding parenchyma of the liver. (D) The shape of the remnant liver parenchyma is the same as in panel B.

Fig. 2 The methods to define the right and ventral margins are shown. (A) IVC and RHV can be identified after hiding the hepatic parenchyma other than the caudate lobe. (B) RHV-IVC plane can be seen (translucent brown) by connecting the RHV from the root + 3 cm and the right border of the IVC. (C) RHV-IVC plane can be seen (yellow) by connecting the RHV from the root + 3 cm and the right border of the IVC. (D) MHV and RHV can be identified after hiding the hepatic parenchyma. (E) MHV-RHV plane can be seen (translucent yellow) by connecting the MHV from the root + 3 cm and RHV from the root + 3 cm. (F) MHV-RHV plane can be seen (yellow) by connecting the MHV from the root + 3 cm and RHV from the root + 3 cm. IVC, inferior vena cava; RHV, right hepatic vein; MHV, middle hepatic vein.

Fig. 3 Right and ventral margins of the caudate lobe are shown. The relations between the caudate lobe and right hepatic vein and inferior vena cava (RHV-IVC) plane and the middle and right hepatic veins (MHV-RHV) plane is shown in Synapse 3-dimensional images. (A) Caudate lobe is located on the right side of the RHV-IVC plane (yellow). (B) The parenchyma of the caudate lobe exceeds the RHV-IVC plane (yellow) is outlined in red. We calculated that the distance exceeds the right margin is 5.6 mm in this case. (C) Caudate lobe is ventrally located in the MHV-RHV plane (yellow). (D) The parenchyma of the caudate lobe exceeds the MHV-RHV plane (yellow) is outlined in red. We calculated that the distance exceeds the ventral margin is 10.6 mm. IVC, inferior vena cava; RHV, right hepatic vein; MHV, middle hepatic vein.
Reference
-
1. Mizumoto R, Kawarada Y, Suzuki H. Surgical treatment of hilar carcinoma of the bile duct. Surg Gynecol Obstet. 1986; 162:153–158.2. Malhi H, Gores GJ. Cholangiocarcinoma: modern advances in understanding a deadly old disease. J Hepatol. 2006; 45:856–867.
Article3. Baton O, Azoulay D, Adam DV, Castaing D. Major hepatectomy for hilar cholangiocarcinoma type 3 and 4: prognostic factors and longterm outcomes. J Am Coll Surg. 2007; 204:250–260.
Article4. Couinaud C. Liver lobes and segments: notes on the anatomical architecture and surgery of the liver. Presse Med. 1954; 62:709–712.5. Kumon M. Anatomy of the caudate lobe with special reference to portal vein and bile duct. Acta Hepatol Jpn. 1985; 26:1193–1199.
Article6. Kogure K, Kuwano H, Yorifuji H, Ishikawa H, Takata K, Makuuchi M. The caudate processus hepatic vein: a boundary hepatic vein between the caudate lobe and the right liver. Ann Surg. 2008; 247:288–293.7. Kitagawa S, Murakami G, Hata F, Hirata K. Configuration of the right portion of the caudate lobe with special reference to identification of its right margin. Clin Anat. 2000; 13:321–340.
Article8. Maki H, Sakamoto Y, Kawaguchi Y, Akamatsu N, Kaneko J, Arita J, et al. Anatomical boundary between the caudate lobe of the liver and adjacent segments based on three-dimensional analysis for precise resections. J Gastrointest Surg. 2018; 22:1709–1714.
Article9. Couinaud C. Surgical anatomy of the liver revisited. Paris: C. Couinaud;1989.10. Kwon D, Murakami G, Hata F, Wang HJ, Chung MS, Hirata K. Location of the ventral margin of the paracaval portion of the caudate lobe of the human liver with special reference to the configuration of hepatic portal vein branches. Clin Anat. 2002; 15:387–401.
Article11. Takayama T, Tanaka T, Higaki T, Katou K, Teshima Y, Makuuchi M. High dorsal resection of the liver. J Am Coll Surg. 1994; 179:72–75.12. Nimura Y, Hayakawa N, Kamiya J, Kondo S, Shionoya S. Hepatic segmentectomy with caudate lobe resection for bile duct carcinoma of the hepatic hilus. World J Surg. 1990; 14:535–543.
Article13. Lerut J, Gruwez JA, Blumgart LH. Resection of the caudate lobe of the liver. Surg Gynecol Obstet. 1990; 171:160–162.14. Cheung TT. Technical notes on pure laparoscopic isolated caudate lobectomy for patient with liver cancer. Transl Gastroenterol Hepatol. 2016; 1:56.
Article15. Oh D, Kwon CH, Na BG, Lee KW, Cho WT, Lee SH, et al. Surgical techniques for totally laparoscopic caudate lobectomy. J Laparoendosc Adv Surg Tech A. 2016; 26:689–692.
Article16. Lee W, Han HS, Yoon YS, Cho JY, Choi Y, Shin HK, et al. Laparoscopic resection of hilar cholangiocarcinoma. Ann Surg Treat Res. 2015; 89:228–232.
Article17. Murakami G, Hata F. Human liver caudate lobe and liver segment. Anat Sci Int. 2002; 77:211–224.
Article18. Couinaud C. The paracaval segment of the liver. J Hep Bil Pancr Surg. 1994; 1:145–151.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- An Analysis on the Usefulness of Concomitant Procurement of the Caudate Lobe in Living Donor Liver Transplantation Using a Left Lobe Graft
- Giant Hyperplasia of the Caudate Lobe in a Patient with Liver Cirrhosis: Case Report and Literature Review
- Total Laparoscopic Liver Resection for a Metastatic Lesion Located in the Caudate Lobe
- Caudate to right lobe ratio of normal liver by computed tomography
- Temporal Pole Projections to the Ventral Shell Striatal Subterritory in the Primate
