Assessment of Endoscopic Gastric Atrophy according to the Kimura-Takemoto Classification and Its Potential Application in Daily Practice
- Affiliations
-
- 1Department of Internal Medicine, University of Medicine and Pharmacy at Ho Chi Minh City, Vietnam. drquachtd@ump.edu.vn
- 2Department of Gastroenterology, Gia- Dinh People’s Hospital, Ho Chi Minh City, Vietnam.
- 3Health Service Center, Hiroshima University, Higashihiroshima, Hiroshima, Japan.
- KMID: 2455627
- DOI: http://doi.org/10.5946/ce.2019.072
Abstract
- The assessment of endoscopic gastric atrophy (EGA) according to the Kimura-Takemoto classification has been reported to correlate well with histological assessment. Although agreement among beginner endoscopists was less than that among experienced endoscopists, it has been shown that agreement level could markedly improve and remained stable after proper training. Several cohort studies have consistently shown that the severity of EGA at baseline is significantly associated with the presence of advanced precancerous gastric lesions and gastric cancer, as well as the development of gastric cancer in future. Patients with moderate-to-severe EGA still have high risk of gastric cancer even after successful Helicobacter pylori eradication and should be candidates for gastric cancer surveillance. The assessment of EGA, therefore, could be used as a preliminary tool to identify individuals at high risk for gastric cancer. In this paper, we review the agreement on mucosal atrophy assessment between the Kimura-Takemoto classification and histology as well as the potential application of this endoscopic classification to identify precancerous gastric lesions and gastric cancer in daily practice.
Keyword
MeSH Terms
Figure
-
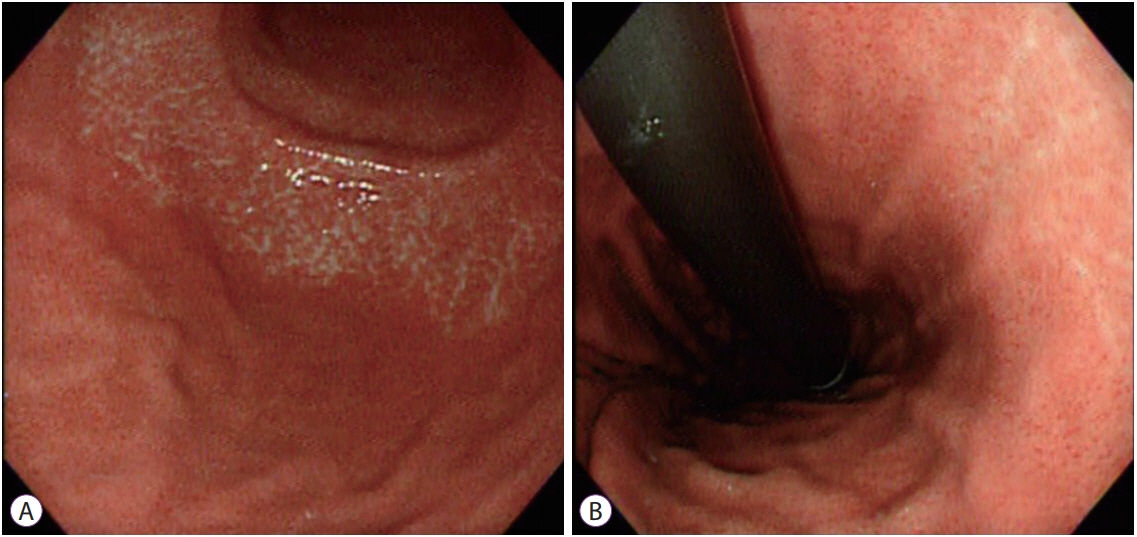
Fig. 1. Atrophic border on the greater curvature (A) and lesser curvature (B). The gastric mucosa shows differences in level and color between the 2 sides of the atrophic border. The endoscopic atrophic border represents both the transition from non-atrophic gastric mucosa to atrophic gastric mucosa and the transition from fundic glands to pyloric glands in a non-atrophic stomach [6]. Its presence, however, does not always mean that a patient has gastric mucosal atrophy. The term “atrophic border” is not accurate and might cause some misunderstanding, but is still used in daily practice due to its historical meaning.
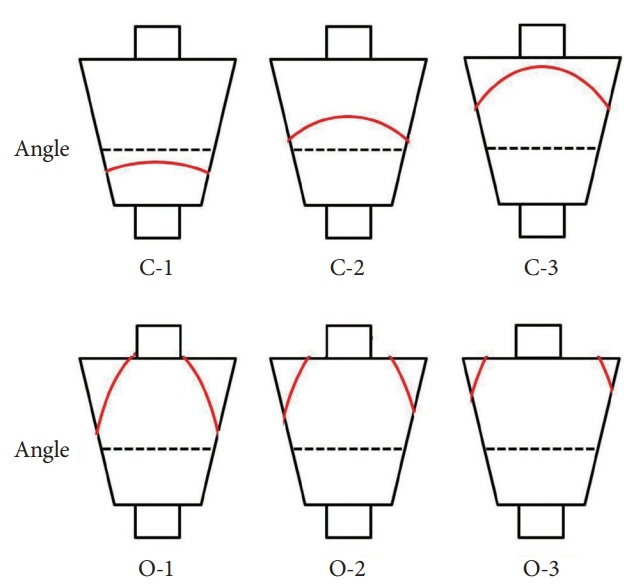
Fig. 2. Extension of the atrophic border (red line) and patterns of endoscopic gastric atrophy as classified by Kimura and Takemoto [13].
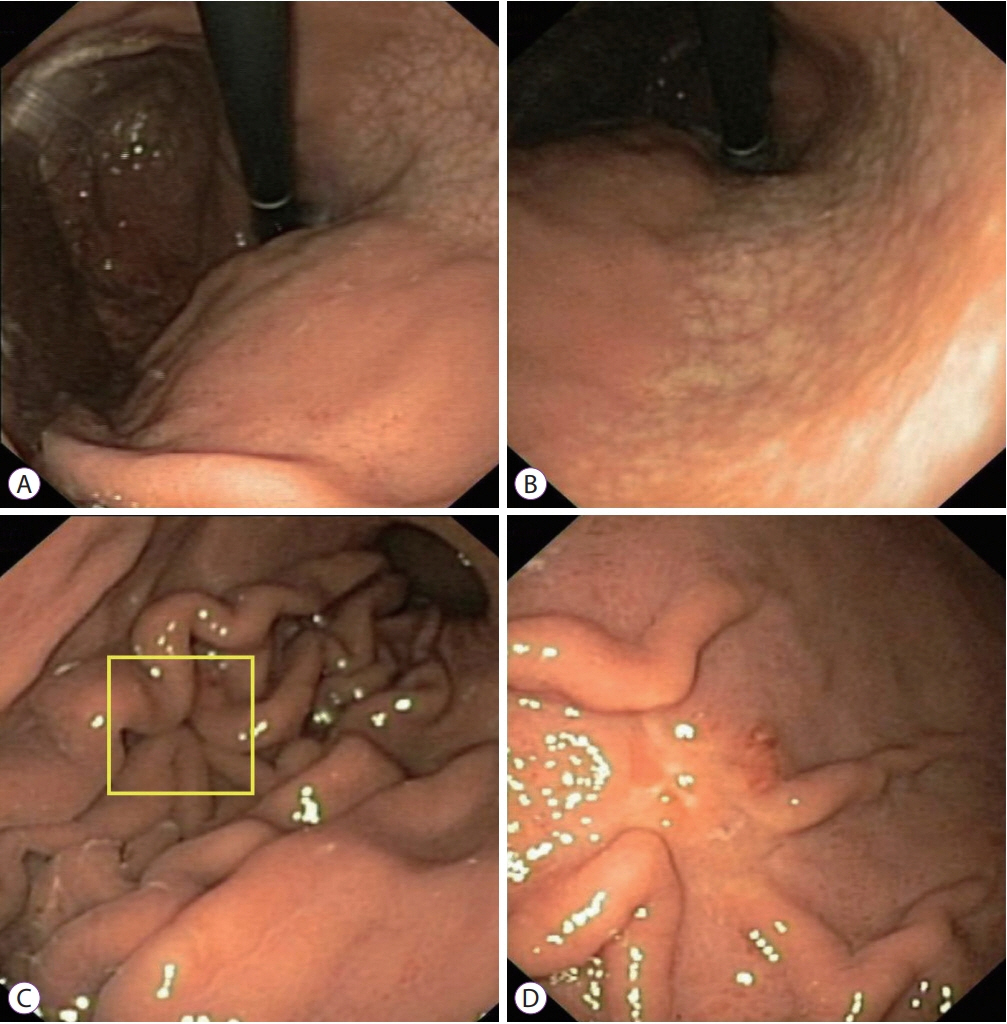
Fig. 3. A 24-year-old Vietnamese female underwent upper gastrointestinal endoscopy for epigastric pain. The patient had no alarming features. (A, B) White-light endoscopy clearly demonstrated moderate endoscopic gastric atrophy (type O-1), even with an older-generation gastroscope (Olympus EXERA-GIF 160 Video Gastroscope; Olympus Co., Tokyo, Japan), which prompted the endoscopist to search carefully for gastric cancer. (C) An easily-missed subtle change (yellow box) could be identified on the greater curvature of the corpus. (D) The gastroscope was advanced closer to the suspicious area and more air was insufflated. A small 0-IIc lesion hidden beneath gastric mucosal folds was identified. This lesion was diagnosed as undifferentiated adenocarcinoma on pathology.
Cited by 1 articles
-
Tauroursodeoxycholic Acid의 위점막 상피세포 NF-κB 신호 전달 억제 및 마우스 위염 예방 효과
Su Hwan Kim, Ji Won Kim, Seong-Joon Koh, Sang Gyun Kim, Jeong Mo Bae, Jung Ho Kim, Jeong Hwan Park, Mee Soo Chang, Kee Don Choi, Hyoun Woo Kang, Byeong Gwan Kim, Kook Lae Lee
Korean J Gastroenterol. 2022;79(4):161-169. doi: 10.4166/kjg.2022.003.
Reference
-
1. Correa P. Helicobacter pylori and gastric carcinogenesis. Am J Surg Pathol. 1995; 19 Suppl 1:S37–S43.2. Rugge M, Meggio A, Pennelli G, et al. Gastritis staging in clinical practice: the OLGA staging system. Gut. 2007; 56:631–636.
Article3. Satoh K, Osawa H, Yoshizawa M, et al. Assessment of atrophic gastritis using the OLGA system. Helicobacter. 2008; 13:225–229.
Article4. Rugge M, Genta RM, Fassan M, et al. OLGA gastritis staging for the prediction of gastric cancer risk: a long-term follow-up study of 7436 patients. Am J Gastroenterol. 2018; 113:1621–1628.
Article5. Rugge M, Meggio A, Pravadelli C, et al. Gastritis staging in the endoscopic follow-up for the secondary prevention of gastric cancer: a 5-year prospective study of 1755 patients. Gut. 2019; 68:11–17.
Article6. Kimura K, Takemoto T. An endoscopic recognition of the atrophic border and its significance in chronic gastritis. Endoscopy. 1969; 1:87–97.
Article7. Dixon MF, Genta RM, Yardley JH, Correa P. Classification and grading of gastritis. The updated Sydney System. International Workshop on the Histopathology of Gastritis, Houston 1994. Am J Surg Pathol. 1996; 20:1161–1181.8. Rugge M, Correa P, Dixon MF, et al. Gastric mucosal atrophy: interobserver consistency using new criteria for classification and grading. Aliment Pharmacol Ther. 2002; 16:1249–1259.
Article9. Correa P. Chronic gastritis: a clinico-pathological classification. Am J Gastroenterol. 1988; 83:504–509.10. Liu Y, Uemura N, Xiao SD, Tytgat GN, Kate FJ. Agreement between endoscopic and histological gastric atrophy scores. J Gastroenterol. 2005; 40:123–127.
Article11. Quach DT, Le HM, Nguyen OT, Nguyen TS, Uemura N. The severity of endoscopic gastric atrophy could help to predict operative link on gastritis assessment gastritis stage. J Gastroenterol Hepatol. 2011; 26:281–285.
Article12. Kono S, Gotoda T, Yoshida S, et al. Can endoscopic atrophy predict histological atrophy? Historical study in United Kingdom and Japan. World J Gastroenterol. 2015; 21:13113–13123.
Article13. Kimura K, Satoh K, Ido K, Taniguchi Y, Takimoto T, Takemoto T. Gastritis in the Japanese stomach. Scand J Gastroenterol Suppl. 1996; 214:17–20. discussion 21-13.
Article14. Andrew A, Wyatt JI, Dixon MF. Observer variation in the assessment of chronic gastritis according to the Sydney system. Histopathology. 1994; 25:317–322.
Article15. Rugge M, Genta RM. Staging gastritis: an international proposal. Gastroenterology. 2005; 129:1807–1808.
Article16. El-Zimaity HM, Ota H, Graham DY, Akamatsu T, Katsuyama T. Patterns of gastric atrophy in intestinal type gastric carcinoma. Cancer. 2002; 94:1428–1436.
Article17. Miwata T, Quach DT, Hiyama T, et al. Interobserver and intraobserver agreement for gastric mucosa atrophy. BMC Gastroenterol. 2015; 15:95.
Article18. Jin EH, Chung SJ, Lim JH, et al. Training effect on the inter-observer agreement in endoscopic diagnosis and grading of atrophic gastritis according to level of endoscopic experience. J Korean Med Sci. 2018; 33:e117.
Article19. Sakaki N, Kozawa H, Egawa N, Tu Y, Sanaka M. Ten-year prospective follow-up study on the relationship between Helicobacter pylori infection and progression of atrophic gastritis, particularly assessed by endoscopic findings. Aliment Pharmacol Ther. 2002; 16 Suppl 2:198–203.
Article20. Kodama M, Okimoto T, Ogawa R, Mizukami K, Murakami K. Endoscopic atrophic classification before and after H. pylori eradication is closely associated with histological atrophy and intestinal metaplasia. Endosc Int Open. 2015; 3:E311–E317.
Article21. Chiu PWY, Uedo N, Singh R, et al. An Asian consensus on standards of diagnostic upper endoscopy for neoplasia. Gut. 2019; 68:186–197.
Article22. Yoshimura T, Shimoyama T, Fukuda S, Tanaka M, Axon AT, Munakata A. Most gastric cancer occurs on the distal side of the endoscopic atrophic border. Scand J Gastroenterol. 1999; 34:1077–1081.
Article23. Tahara T, Shibata T, Horiguchi N, et al. A possible link between gastric mucosal atrophy and gastric cancer after Helicobacter pylori eradication. PLoS One. 2016; 11:e0163700.
Article24. Nishida T, Tsujii M, Kato M, et al. Endoscopic surveillance strategy after endoscopic resection for early gastric cancer. World J Gastrointest Pathophysiol. 2014; 5:100–106.
Article25. Lee HJ, Lee YJ, Lee JY, et al. Characteristics of synchronous and metachronous multiple gastric tumors after endoscopic submucosal dissection of early gastric neoplasm. Clin Endosc. 2018; 51:266–273.
Article26. Masuyama H, Yoshitake N, Sasai T, et al. Relationship between the degree of endoscopic atrophy of the gastric mucosa and carcinogenic risk. Digestion. 2015; 91:30–36.
Article27. Sugano K, Tack J, Kuipers EJ, et al. Kyoto global consensus report on Helicobacter pylori gastritis. Gut. 2015; 64:1353–1367.28. Chen HN, Wang Z, Li X, Zhou ZG. Helicobacter pylori eradication cannot reduce the risk of gastric cancer in patients with intestinal metaplasia and dysplasia: evidence from a meta-analysis. Gastric Cancer. 2016; 19:166–175.
Article29. Kaji K, Hashiba A, Uotani C, et al. Grading of atrophic gastritis is useful for risk stratification in endoscopic screening for gastric cancer. Am J Gastroenterol. 2019; 114:71–79.
Article30. Take S, Mizuno M, Ishiki K, et al. The long-term risk of gastric cancer after the successful eradication of Helicobacter pylori. J Gastroenterol. 2011; 46:318–324.
Article31. Toyoshima O, Yamaji Y, Yoshida S, et al. Endoscopic gastric atrophy is strongly associated with gastric cancer development after Helicobacter pylori eradication. Surg Endosc. 2017; 31:2140–2148.
Article32. Shichijo S, Hirata Y. Characteristics and predictors of gastric cancer after Helicobacter pylori eradication. World J Gastroenterol. 2018; 24:2163–2172.
Article33. Sakitani K, Hirata Y, Suzuki N, et al. Gastric cancer diagnosed after Helicobacter pylori eradication in diabetes mellitus patients. BMC Gastroenterol. 2015; 15:143.
Article34. Kodama M, Murakami K, Okimoto T, et al. Histological characteristics of gastric mucosa prior to Helicobacter pylori eradication may predict gastric cancer. Scand J Gastroenterol. 2013; 48:1249–1256.35. Sekikawa A, Fukui H, Sada R, et al. Gastric atrophy and xanthelasma are markers for predicting the development of early gastric cancer. J Gastroenterol. 2016; 51:35–42.
Article36. Sugimoto M, Ban H, Ichikawa H, et al. Efficacy of the Kyoto classification of gastritis in identifying patients at high risk for gastric cancer. Intern Med. 2017; 56:579–586.
Article37. Shichijo S, Hirata Y, Niikura R, et al. Histologic intestinal metaplasia and endoscopic atrophy are predictors of gastric cancer development after Helicobacter pylori eradication. Gastrointest Endosc. 2016; 84:618–624.
Article38. Uemura N, Okamoto S, Yamamoto S, et al. Helicobacter pylori infection and the development of gastric cancer. N Engl J Med. 2001; 345:784–789.39. Hosokawa O, Watanabe K, Hatorri M, Douden K, Hayashi H, Kaizaki Y. Detection of gastric cancer by repeat endoscopy within a short time after negative examination. Endoscopy. 2001; 33:301–305.
Article40. Majima A, Handa O, Naito Y, et al. Early-stage gastric cancer can be found in improved atrophic mucosa over time from successful Helicobacter pylori eradication. Digestion. 2017; 95:194–200.41. Fukase K, Kato M, Kikuchi S, et al. Effect of eradication of Helicobacter pylori on incidence of metachronous gastric carcinoma after endoscopic resection of early gastric cancer: an open-label, randomised controlled trial. Lancet. 2008; 372:392–397.
Article42. Mori G, Nakajima T, Asada K, et al. Incidence of and risk factors for metachronous gastric cancer after endoscopic resection and successful Helicobacter pylori eradication: results of a large-scale, multicenter cohort study in Japan. Gastric Cancer. 2016; 19:911–918.
Article43. Nam HS, Kim HW, Choi CW, et al. Characteristics of overlooked synchronous gastric epithelial neoplasia after endoscopic submucosal dissection. Medicine (Baltimore). 2018; 97:e12536.
Article44. Quach DT, Le HM, Hiyama T, Nguyen OT, Nguyen TS, Uemura N. Relationship between endoscopic and histologic gastric atrophy and intestinal metaplasia. Helicobacter. 2013; 18:151–157.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endoscopic Diagnosis and Classification of Atrophic Gastritis and Intestinal Metaplasia
- History of Various Classifications of Gastritis
- Endoscopic Findings of Common Gastritis in Koreans
- Clinical Application of the Kyoto Classification of Gastritis
- Effectiveness of Helicobacter pylori Eradication before Endoscopic Resection
