First Metatarsal Proximal Opening Wedge Osteotomy for Correction of Hallux Valgus Deformity: Comparison of Straight versus Oblique Osteotomy
- Affiliations
-
- 1Department of Orthopaedic Surgery, Yonsei University College of Medicine, Seoul, Korea.
- 2Department of Orthopaedic Surgery, Yonsei Altair Hospital, Seoul, Korea.
- 3Department of Orthopaedic Surgery, Yonsei Sarang Hospital, Seoul, Korea. yskimos@gmail.com
- KMID: 2450349
- DOI: http://doi.org/10.3349/ymj.2015.56.3.744
Abstract
- PURPOSE
The aim of this study was to compare clinical and radiographic outcomes of proximal opening wedge osteotomy using a straight versus oblique osteotomy.
MATERIALS AND METHODS
We retrospectively reviewed 104 consecutive first metatarsal proximal opening wedge osteotomies performed in 95 patients with hallux valgus deformity. Twenty-six feet were treated using straight metatarsal osteotomy (group A), whereas 78 feet were treated using oblique metatarsal osteotomy (group B). The hallux valgus angle (HVA), intermetatarsal angle (IMA), distal metatarsal articular angle, and distance from the first to the second metatarsal (distance) were measured for radiographic evaluation, whereas the American Orthopaedic Foot and Ankle Society (AOFAS) forefoot score was used for clinical evaluation.
RESULTS
Significant corrections in the HVA, IMA, and distance from the first to the second metatarsal were obtained in both groups at the last follow-up (p<0.001). There was no difference in the mean IMA correction between the 2 groups (6.1+/-2.7degrees in group A and 6.0+/-2.1degrees in group B). However, a greater correction in the HVA and distance from the first to the second metatarsal were found in group B (HVA, 13.2+/-8.2degrees; distance, 25.1+/-0.2 mm) compared to group A (HVA, 20.9+/-7.7degrees; distance, 28.1+/-0.3 mm; p<0.001). AOFAS scores were improved in both groups. However, group B demonstrated a greater improvement relative to group A (p=0.005).
CONCLUSION
Compared with a straight first metatarsal osteotomy, an oblique first metatarsal osteotomy yielded better clinical and radiological outcomes.
MeSH Terms
-
Adult
Aged
Bone Plates
Epiphyses/surgery
Ethnic Groups
Female
Foot
Fracture Fixation, Internal/*instrumentation
Hallux Valgus/radiography/*surgery
Humans
Lower Extremity
Male
Metatarsal Bones/*radiography/*surgery
Middle Aged
Osteotomy/*methods
Range of Motion, Articular
Retrospective Studies
Treatment Outcome
Upper Extremity
Figure
-
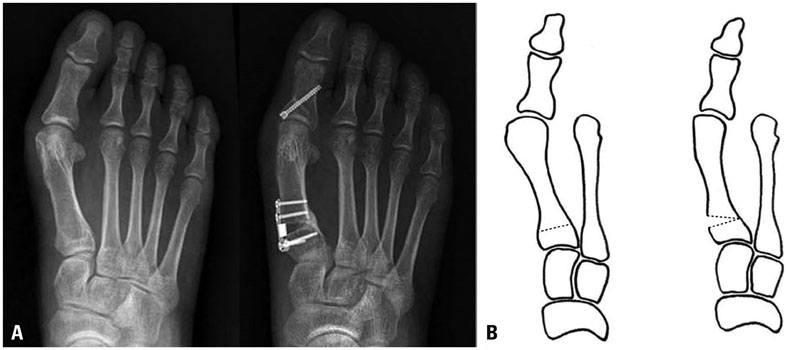
Fig. 1 Preoperative (left) and 3-month postoperative (right) weight-bearing anteroposterior radiographs (A) and schematic drawings (B) of a proximal opening wedge osteotomy utilizing a straight osteotomy. Although the intermetatarsal angle was corrected after surgery, the distance from the first to the second metatarsal was not significantly decreased, and the hallux valgus angle was not corrected.
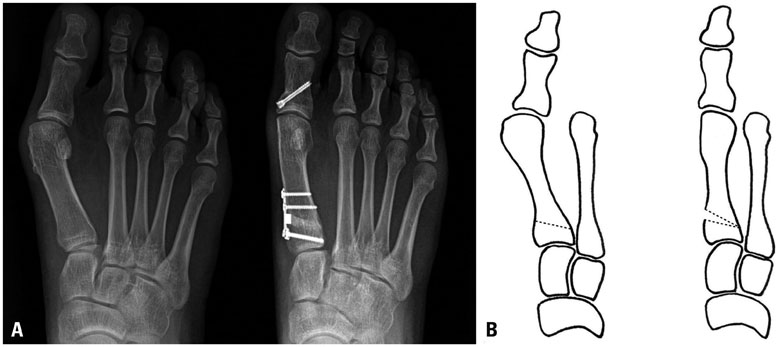
Fig. 2 Preoperative (left) and 12-month postoperative (right) weight-bearing anteroposterior radiographs (A) and schematic drawings (B) of a proximal opening wedge osteotomy utilizing an oblique osteotomy. After surgery, the intermetatarsal angle and hallux valgus angle were corrected, and the distance from the first to the second metatarsal was decreased.
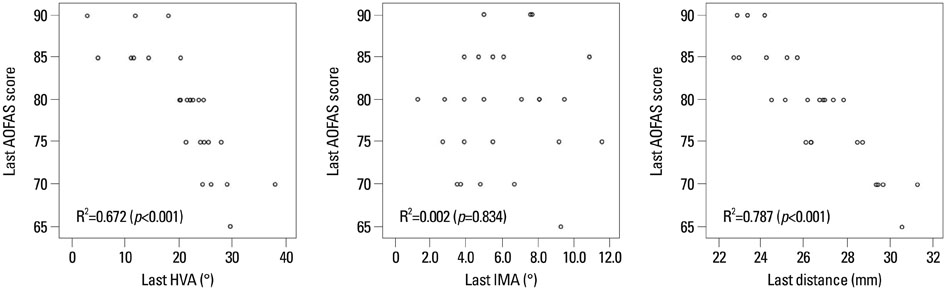
Fig. 3 Associations between the American Orthopaedic Foot and Ankle Society (AOFAS) score and final follow-up radiographic outcomes, including the hallux valgus angle (HVA), intermetatarsal angle (IMA), and distance from the first to the second metatarsal (distance), in group A.
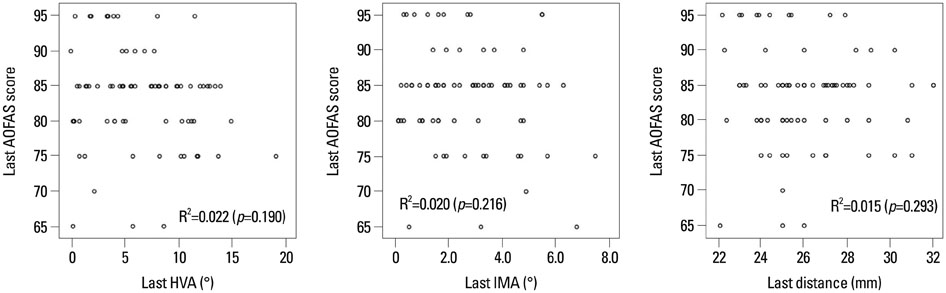
Fig. 4 Associations between the American Orthopaedic Foot and Ankle Society (AOFAS) score and final follow-up radiographic outcomes, including the hallux valgus angle (HVA), intermetatarsal angle (IMA), and distance from the first to the second metatarsal (distance), in group B.
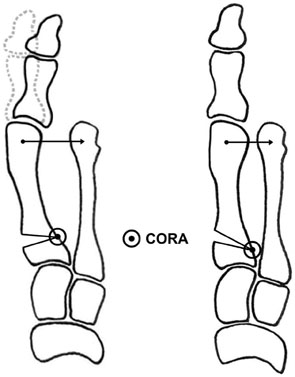
Fig. 5 In an oblique osteotomy (right), the center of rotation of angulation (CORA) is located more proximally and closer to the second metatarsal base than in a straight osteotomy (left). Thus, the distance from the first to the second metatarsal decreases more in an oblique osteotomy than in a straight osteotomy. In a straight osteotomy, correction of the hallux valgus angle (dotted line) is decreased because of the wide distance from the first to the second metatarsal.
Cited by 1 articles
-
Point-Connecting Measurements of the Hallux Valgus Deformity: A New Measurement and Its Clinical Application
Jeong-Ho Seo, Ji-Yong Ahn, Dimas Boedijono
Yonsei Med J. 2016;57(3):741-747. doi: 10.3349/ymj.2016.57.3.741.
Reference
-
1. Kummer FJ. Mathematical analysis of first metatarsal osteotomies. Foot Ankle. 1989; 9:281–289.
Article2. Easley ME, Kiebzak GM, Davis WH, Anderson RB. Prospective, randomized comparison of proximal crescentic and proximal chevron osteotomies for correction of hallux valgus deformity. Foot Ankle Int. 1996; 17:307–316.
Article3. Schwartz N, Groves ER. Long-term follow-up of internal threaded Kirschner-wire fixation of the scarf bunionectomy. J Foot Surg. 1987; 26:313–316.4. Saxena A, McCammon D. The Ludloff osteotomy: a critical analysis. J Foot Ankle Surg. 1997; 36:100–105.
Article5. Campbell JT, Schon LC, Parks BG, Wang Y, Berger BI. Mechanical comparison of biplanar proximal closing wedge osteotomy with plantar plate fixation versus crescentic osteotomy with screw fixation for the correction of metatarsus primus varus. Foot Ankle Int. 1998; 19:293–299.
Article6. Neese DJ, Zelichowski JE, Patton GW. Mau osteotomy: an alternative procedure to the closing abductory base wedge osteotomy. J Foot Surg. 1989; 28:352–362.7. Thordarson DB, Leventen EO. Hallux valgus correction with proximal metatarsal osteotomy: two-year follow-up. Foot Ankle. 1992; 13:321–326.
Article8. Choi WJ, Yoon HK, Yoon HS, Kim BS, Lee JW. Comparison of the proximal chevron and Ludloff osteotomies for the correction of hallux valgus. Foot Ankle Int. 2009; 30:1154–1160.
Article9. Trethowan J. Hallux Valgus. In : Choyce CC, editor. A system of surgery. New York: PB Hoeber;1923. p. 1046–1049.10. Coughlin MJ. Hallux valgus. J Bone Joint Surg Am. 1996; 78:932–966.11. Cooper MT, Berlet GC, Shurnas PS, Lee TH. Proximal opening-wedge osteotomy of the first metatarsal for correction of hallux valgus. Surg Technol Int. 2007; 16:215–219.12. Shurnas PS, Watson TS, Crislip TW. Proximal first metatarsal opening wedge osteotomy with a low profile plate. Foot Ankle Int. 2009; 30:865–872.
Article13. Saragas NP. Proximal opening-wedge osteotomy of the first metatarsal for hallux valgus using a low profile plate. Foot Ankle Int. 2009; 30:976–980.
Article14. Randhawa S, Pepper D. Radiographic evaluation of hallux valgus treated with opening wedge osteotomy. Foot Ankle Int. 2009; 30:427–431.
Article15. Park CH, Ahn JY, Kim YM, Lee WC. Plate fixation for proximal chevron osteotomy has greater risk for hallux valgus recurrence than Kirschner wire fixation. Int Orthop. 2013; 37:1085–1092.
Article16. Schneider W, Csepan R, Knahr K. Reproducibility of the radiographic metatarsophalangeal angle in hallux surgery. J Bone Joint Surg Am. 2003; 85-A:494–499.
Article17. Smith BW, Coughlin MJ. Treatment of hallux valgus with increased distal metatarsal articular angle: use of double and triple osteotomies. Foot Ankle Clin. 2009; 14:369–382.
Article18. Kitaoka HB, Alexander IJ, Adelaar RS, Nunley JA, Myerson MS, Sanders M. Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int. 1994; 15:349–353.
Article19. Watson TS, Shurnas PS. The proximal opening wedge osteotomy for the correction of hallux valgus deformity. Tech Foot Ankle Surg. 2012; 11:168–174.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Clinical Results of the Proximal Opening Wedge Osteotomy Using a Low Profile Plate in Hallux Valgus: Comparison with Proximal Chevron Osteotomy Fixed with K-wires
- A Comparison of Operative Treatment of Hallux Valgus with a Proximal Metatarsal Osteotomy and with a Modified Chevron Osteotomy
- Minimally Invasive Proximal Transverse Metatarsal Osteotomy Followed by Intramedullary Plate Fixation for Hallux Valgus Deformity: A Case Report
- Comparison of the Results between Distal Chevron Osteotomy and Proximal Metatarsal Osteotomy for the Treatment of Moderate Hallux Valgus
- Chevron Osteotomy as the Treatment of Moderate to Severe Hallux Valgus Deformity
