Allergy Asthma Immunol Res.
2019 Jul;11(4):538-547. 10.4168/aair.2019.11.4.538.
Cold Urticaria: Clinical Features and Natural Course in a Tropical Country
- Affiliations
-
- 1Department of Dermatology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand. kanokvalai.kul@mahidol.ac.th
- KMID: 2448756
- DOI: http://doi.org/10.4168/aair.2019.11.4.538
Abstract
- PURPOSE
To review the clinical features and natural courses of cold urticaria (ColdU) in a tropical country.
METHODS
A retrospective chart review was performed of patients who visited Siriraj Urticaria Clinic, Siriraj Hospital, Bangkok, Thailand, and were diagnosed with ColdU between 2007 and 2018. Data on provocation and threshold tests, clinical courses, and laboratory work-up were analyzed and compared with data reported by studies in temperate countries.
RESULTS
Of 1,063 chronic urticaria patients, 27 (2.5%) were diagnosed with ColdU, with a mean age of symptom onset of 34.8 years. Half of the patients had a history of atopy, and 1 (3.7%) had a history of anaphylaxis. All patients were positive to 1 of 3 provocation tests: an ice cube test; TempTest 4.0; or a tray filled with ice, salt and water. Thirteen patients underwent the ice cube test, and all had positive results. TempTest was performed on 15 patients, 8 of whom had positive results, with a mean critical temperature threshold (CTT) of 21.0°C. All of the 7 patients who had a negative TempTest result later produced positive results to the immersion of their hand and forearm in a tray filled with ice, salt, and water. All patients were treated with H1-antihistamines, the vast majority (96.3%) being non-sedating H1-antihistamines. Some (14.8%) needed to be administered oral corticosteroids, ciclosporin, or omalizumab. Six patients (22.2%) were in remission. A Kaplan-Meier survival curve demonstrated 5-year and 10-year remission rates of 13.8% and 42.6%, respectively.
CONCLUSIONS
The rate of anaphylaxis in patients with ColdU in a tropical country was lower than those reported by other studies conducted intemperate climates. On the other hand, the number of female patients, mean age at symptom onset, atopy rate, rate of concomitant chronic spontaneous urticaria and mean CTT were higher.
MeSH Terms
Figure
-
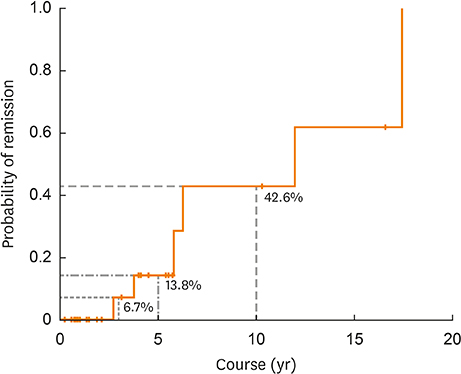
Figure A Kaplan-Meier survival analysis (one minus survival function) demonstrating the duration of ColdU (n = 27). None of the patients were in remission during the first 2 years of the disease. However, after 3, 5 and 10 years from the onset of symptoms, 6.7%, 13.8%, and 42.6% of ColdU patients, respectively, were in remission. The median duration, when 50% of patients were in remission, was 12 years. ColdU, cold urticaria.
Reference
-
1. Magerl M, Altrichter S, Borzova E, Giménez-Arnau A, Grattan CE, Lawlor F, et al. The definition, diagnostic testing, and management of chronic inducible urticarias - the EAACI/GA2LEN/EDF/UNEV consensus recommendations 2016 update and revision. Allergy. 2016; 71:780–802.2. Maurer M, Fluhr JW, Khan DA. How to approach chronic inducible urticaria. J Allergy Clin Immunol Pract. 2018; 6:1119–1130.
Article3. Deza G, Brasileiro A, Bertolín-Colilla M, Curto-Barredo L, Pujol RM, Giménez-Arnau AM. Acquired cold urticaria: clinical features, particular phenotypes, and disease course in a tertiary care center cohort. J Am Acad Dermatol. 2016; 75:918–924.e2.
Article4. Trevisonno J, Balram B, Netchiporouk E, Ben-Shoshan M. Physical urticaria: review on classification, triggers and management with special focus on prevalence including a meta-analysis. Postgrad Med. 2015; 127:565–570.
Article5. Möller A, Henning M, Zuberbier T, Czarnetzki-Henz BM. Epidemiology and clinical aspects of cold urticaria. Hautarzt. 1996; 47:510–514.6. Katsarou-Katsari A, Makris M, Lagogianni E, Gregoriou S, Theoharides T, Kalogeromitros D. Clinical features and natural history of acquired cold urticaria in a tertiary referral hospital: a 10-year prospective study. J Eur Acad Dermatol Venereol. 2008; 22:1405–1411.
Article7. Kozel MM, Mekkes JR, Bossuyt PM, Bos JD. Natural course of physical and chronic urticaria and angioedema in 220 patients. J Am Acad Dermatol. 2001; 45:387–391.
Article8. Ferrer M. Epidemiology, healthcare, resources, use and clinical features of different types of urticaria. Alergológica 2005. J Investig Allergol Clin Immunol. 2009; 19:Suppl 2. 21–26.9. Sibbald RG, Cheema AS, Lozinski A, Tarlo S. Chronic urticaria. Evaluation of the role of physical, immunologic, and other contributory factors. Int J Dermatol. 1991; 30:381–386.10. Siebenhaar F, Staubach P, Metz M, Magerl M, Jung J, Maurer M. Peltier effect-based temperature challenge: an improved method for diagnosing cold urticaria. J Allergy Clin Immunol. 2004; 114:1224–1225.
Article11. Claudy A. Cold urticaria. J Investig Dermatol Symp Proc. 2001; 6:141–142.
Article12. Visitsunthorn N, Tuchinda M, Vichyanond P. Cold urticaria in Thai children: comparison between cyproheptadine and ketotifen in the treatment. Asian Pac J Allergy Immunol. 1995; 13:29–35.13. Neittaanmäki H, Myöhänen T, Fräki JE. Comparison of cinnarizine, cyproheptadine, doxepin, and hydroxyzine in treatment of idiopathic cold urticaria: usefulness of doxepin. J Am Acad Dermatol. 1984; 11:483–489.
Article14. Metz M, Schütz A, Weller K, Gorczyza M, Zimmer S, Staubach P, et al. Omalizumab is effective in cold urticaria-results of a randomized placebo-controlled trial. J Allergy Clin Immunol. 2017; 140:864–867.e5.
Article15. Jain SV, Mullins RJ. Cold urticaria: a 20-year follow-up study. J Eur Acad Dermatol Venereol. 2016; 30:2066–2071.
Article16. Neittaanmäki H. Cold urticaria. Clinical findings in 220 patients. J Am Acad Dermatol. 1985; 13:636–644.17. Silpa-archa N, Kulthanan K, Pinkaew S. Physical urticaria: prevalence, type and natural course in a tropical country. J Eur Acad Dermatol Venereol. 2011; 25:1194–1199.
Article18. Boonpiyathad T, Sangasapaviliya A. Autologous serum and plasma skin test to predict 2-year outcome in chronic spontaneous urticaria. Asia Pac Allergy. 2016; 6:226–235.
Article19. Kulthanan K, Jiamton S, Thumpimukvatana N, Pinkaew S. Chronic idiopathic urticaria: prevalence and clinical course. J Dermatol. 2007; 34:294–301.
Article20. Wanderer AA, Grandel KE, Wasserman SI, Farr RS. Clinical characteristics of cold-induced systemic reactions in acquired cold urticaria syndromes: recommendations for prevention of this complication and a proposal for a diagnostic classification of cold urticaria. J Allergy Clin Immunol. 1986; 78:417–423.
Article21. Vichyanond P, Sunthornchart S, Singhirannusorn V, Ruangrat S, Kaewsomboon S, Visitsunthorn N. Prevalence of asthma, allergic rhinitis and eczema among university students in Bangkok. Respir Med. 2002; 96:34–38.
Article22. Kim JS, Yethiraj A. The effect of salt on the melting of ice: a molecular dynamics simulation study. J Chem Phys. 2008; 129:124504.
Article23. Grattan CE, Sabroe RA, Greaves MW. Chronic urticaria. J Am Acad Dermatol. 2002; 46:645–657.
Article
