Gallbladder Fistula Treated with N-Butyl-2-Cyanoacrylate after Radiofrequency Ablation in a Hepatocellular Carcinoma Patient: a Case Report
- Affiliations
-
- 1Department of Internal Medicine, Keimyung University School of Medicine, Daegu, Korea. gastro@dsmc.or.kr
- 2Department of Radiology, Daegu Catholic University Medical Center, Catholic University of Daegu College of Medicine, Daegu, Korea.
- KMID: 2448280
- DOI: http://doi.org/10.17998/jlc.19.1.69
Abstract
- Radiofrequency ablation (RFA) is a minimally invasive local therapy for hepatocellular carcinoma (HCC). Even though RFA is considered to be a safe treatment modality, a variety of complications have been reported. Recently, we encountered a case of refractory fistula between a liver abscess and the gallbladder after RFA. A 64-year-old woman diagnosed with HCC associated with chronic hepatitis B was treated by RFA. After RFA, she experienced abdominal pain, and abdominal computed tomography (CT) revealed a liver abscess complicated by a previous treatment of HCC, she was treated with intravenous antibiotics and percutaneous abscess drainage. Follow-up abdominal CT revealed a fistula between the liver abscess and gallbladder, which was successfully treated with percutaneous transcatheter n-butyl-2-cyanoacrylate (NBCA) embolization. We herein report the rare case of a refractory fistula between a liver abscess and the gallbladder after RFA in a patient treated with NBCA embolization.
MeSH Terms
Figure
-
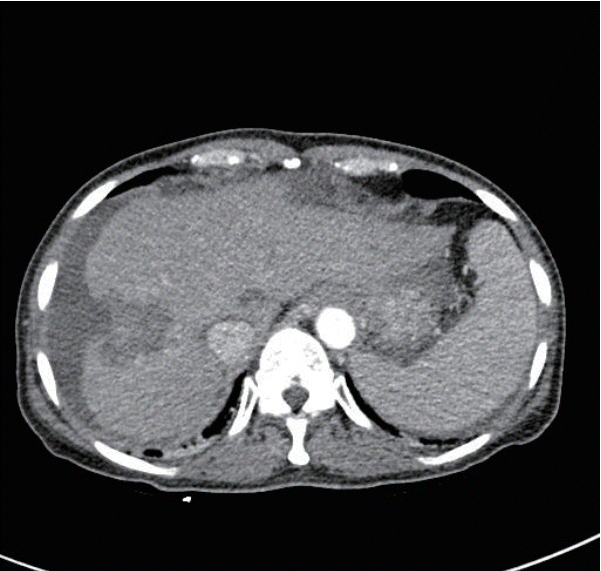
Figure 1. Dynamic CT during arterial phase showing an ill-defined, irregularly shaped liver abscess in the right anterior, superior segment of the liver and perihepatic fluid collection. CT, computed tomography.
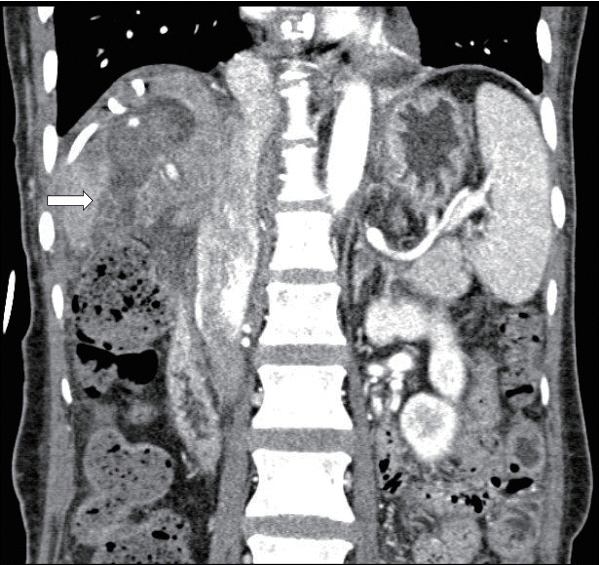
Figure 2. Dynamic CT showing an abscess and gallbladder fistula (white arrow). CT, computed tomography.
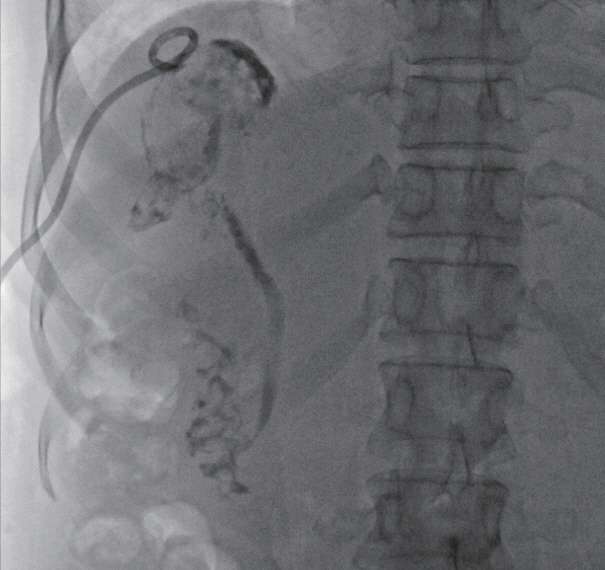
Figure 3. Tubography via a pigtail catheter showing the passage of the contrast dye through the gallbladder, cystic duct, common bile duct, and duodenum due to fistula formation between the abscess and gallbladder.
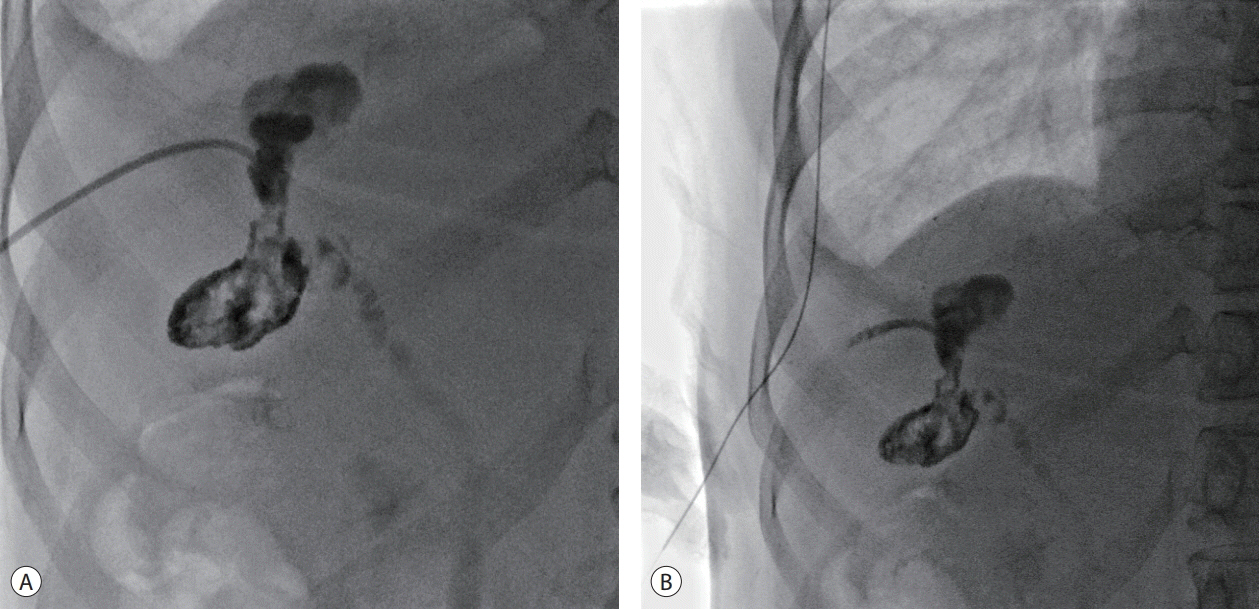
Figure 4. (A) Tubography showing fistula embolization with an NBCA-lipiodol mixture, and NBCA is observed along the previous remnant abscess, fistula tract, and gallbladder. (B) After the fistula tract embolization procedure, the percutaneous drainage catheter was removed. NBCA, n-butyl-2-cyanoacrylate.

Figure 5. CT showing the remnant abscess, fistula tract, and gallbladder cavity sealed with NBCA. CT, computed tomography; NBCA, n-butyl-2-cyanoacrylate.

Figure 6. Tubography showing the fistula tract occlusion through non-visualization of the cystic duct, common bile duct, and duodenum after dyeinjection.
Reference
-
1. Bruix J, Llovet JM. Prognostic prediction and treatment strategy in hepatocellular carcinoma. Hepatology. 2002; 35:519–524.2. Rossi S, Buscarini E, Garbagnati F, Di Stasi M, Quaretti P, Rago M, et al. Percutaneous treatment of small hepatic tumors by an expandable RF needle electrode. AJR Am J Roentgenol. 1998; 170:1015–1022.3. Bai XM, Yang W, Zhang ZY, Jiang AN, Wu W, Lee JC, et al. Longterm outcomes and prognostic analysis of percutaneous radiofrequency ablation in liver metastasis from breast cancer. Int J Hyperthermia. 2019; 35:183–193.4. Livraghi T, Solbiati L, Meloni MF, Gazelle GS, Halpern EF, Goldberg SN. Treatment of focal liver tumors with percutaneous radio-frequency ablation: complications encountered in a multicenter study. Radiology. 2003; 226:441–451.5. Rhim H, Yoon KH, Lee JM, Cho Y, Cho JS, Kim SH, et al. Major complications after radio-frequency thermal ablation of hepatic tumors: spectrum of imaging findings. Radiographics. 2003; 23:123–134. ; discussion 134-136.6. Bertot LC, Sato M, Tateishi R, Yoshida H, Koike K. Mortality and complication rates of percutaneous ablative techniques for the treatment of liver tumors: a systematic review. Eur Radiol. 2011; 21:2584–2596.7. Bae JH, Kim GC, Ryeom HK, Jang YJ. Percutaneous embolization of persistent biliary and enteric fistulas with Histoacryl. J Vasc Interv Radiol. 2011; 22:879–883.8. York JA. Treating bronchopleural fistulae percutaneously with Nbutyl cyanoacrylate glue. J Vasc Interv Radiol. 2013; 24:1581–1583.9. Nunes TF, de Santi GF. Percutaneous embolization of a colonic fistula using n-butyl-2 cyanoacrylate (Histoacryl[R]). Tech Coloproctol. 2017; 21:763–765.10. Lopes MF, Catré D, Reis A, Leitão LM. Endoscopic treatment of recurrent tracheoesophageal fistula with histoacryl glue. Gastrointest Endosc. 2010; 72:1324–1325. ; author reply 1325.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Abscesso-Colonic Fistula Following Radiofrequency Ablation Therapy for Hepatocellular Carcinoma; A Case Successfully Treated with Histoacryl Embolization
- N-Butyl Cyanoacrylate Embolization with Blood Flow Control of an Arterioportal Shunt That Developed after Radiofrequency Ablation of Hepatocellular Carcinoma
- Biliary Fistula Developed after Radiofrequency Ablation Therapy for Hepatocellular Carcinoma
- Biliary-duodenal Fistula Following Radiofrequency Ablation Therapy for Hepatocellular Carcinoma
- Hepatocolic Fistula after Radiofrequency Ablation for Hepatocellular Carcinoma
