N-Butyl Cyanoacrylate Embolization with Blood Flow Control of an Arterioportal Shunt That Developed after Radiofrequency Ablation of Hepatocellular Carcinoma
- Affiliations
-
- 1Department of Radiology, Wakayama Medical University, Wakayama 641-8510, Japan. sonomura@wakayama-med.ac.jp
- 2Department of Internal Medicine, Wakayama Medical University, Wakayama 641-8510, Japan.
- KMID: 1705580
- DOI: http://doi.org/10.3348/kjr.2014.15.2.250
Abstract
- We present a case of a patient with rapid deterioration of esophageal varices caused by portal hypertension accompanied by a large arterioportal shunt that developed after radiofrequency ablation of hepatocellular carcinoma. We used n-butyl cyanoacrylate (NBCA) as an embolic material to achieve pinpoint embolization of the shunt, because the microcatheter tip was 2 cm away from the shunt site. Under hepatic arterial flow control using a balloon catheter, the arterioportal shunt was successfully embolized with NBCA, which caused an improvement in the esophageal varices.
Keyword
MeSH Terms
-
Aged
Arteriovenous Fistula/etiology/radiography/*therapy
Carcinoma, Hepatocellular/*surgery
Catheter Ablation/*adverse effects
Embolization, Therapeutic/*methods
Enbucrilate/*therapeutic use
Esophageal and Gastric Varices/etiology/*therapy
Hepatic Artery/*abnormalities/radiography
Humans
Liver Neoplasms/*surgery
Male
Portal Vein/*abnormalities/radiography
Enbucrilate
Figure
-
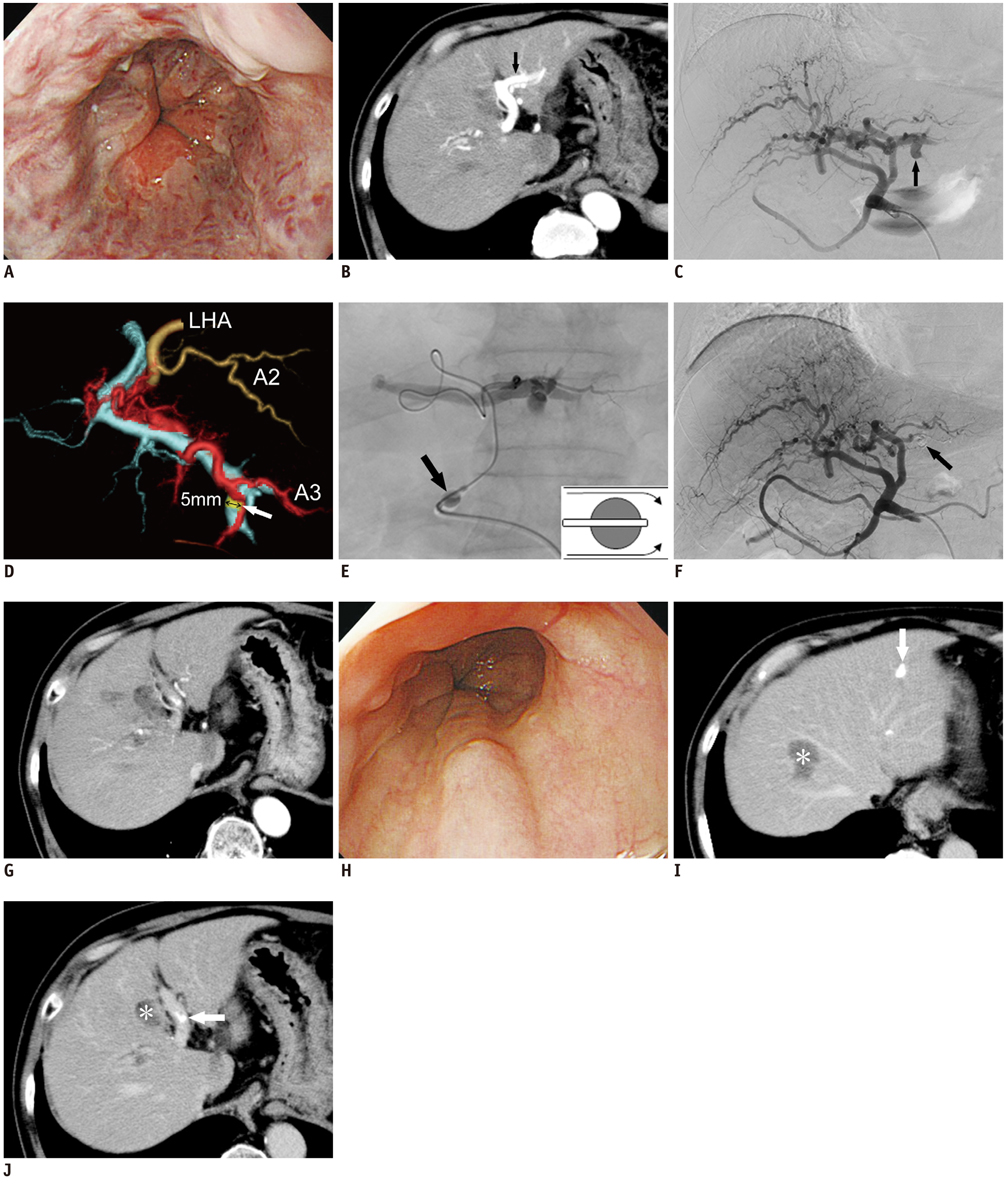
Fig. 1 N-butyl cyanoacrylate (NBCA) embolization of arterioportal shunt under blood flow control with balloon catheter. A. Endoscopy before embolization revealed large red-colored esophageal varices. B. Arterial phase contrast-enhanced computed tomography performed before embolization revealed early enhancement of left portal vein (arrow), suggesting presence of arterioportal shunt. C. Angiography performed before embolization revealed presence of large arterioportal shunt (arrow) in left lateral segment of liver. D. Volume-rendered images from computed tomography performed during hepatic arteriography. Superior view showed that shunt site (yellow) was 5 mm in diameter (arrow), and was located between hepatic artery (red) and portal vein (light blue) in segment 3 of liver. E. NBCA mixture was injected through 2-Fr microcatheter that was advanced as close as possible to arterioportal shunt under blood flow control using balloon catheter (arrow) that was inserted in proper hepatic artery. Balloon was used to incompletely occlude artery, allowing antegrade blood flow (inset at bottom right). F. Angiography performed after embolization showed complete disappearance of shunt and presence of NBCA mixture at shunt site (arrow). LHA = left hepatic artery. G. Contrast-enhanced computed tomography (CE-CT) after embolization showed complete disappearance of shunt. H. Endoscopy performed at 6 months after embolization confirmed that varices had shrunk and red color sign had disappeared. I, J. CE-CT performed at 6 months after embolization revealed presence of NBCA mixture at shunt site in segment 3 of liver, and in left portal vein (arrows). Necrotic lesions (asterisks) caused by radiofrequency ablation were found in segments 8 and 4 of liver.
Reference
-
1. Livraghi T, Solbiati L, Meloni MF, Gazelle GS, Halpern EF, Goldberg SN. Treatment of focal liver tumors with percutaneous radio-frequency ablation: complications encountered in a multicenter study. Radiology. 2003; 226:441–451.2. Lazaridis KN, Kamath PS. Images in hepatology. Arterioportal fistula causing recurrent variceal bleeding. J Hepatol. 1998; 29:142.3. Kerlan RK Jr, Bank WO, Hoddick WK, Pogany AC, Sollenberger RD. Occlusion of a hepatic artery to portal vein fistula with bucrylate. Cardiovasc Intervent Radiol. 1983; 6:138–140.4. Kanematsu M, Kondo H, Goshima S, Tsuge Y, Watanabe H, Moriyama N. Giant high-flow type pulmonary arteriovenous malformation: coil embolization with flow control by balloon occlusion and an anchored detachable coil. Korean J Radiol. 2012; 13:111–114.5. Idezuki Y. Japanese Society for Portal Hypertension. General rules for recording endoscopic findings of esophagogastric varices (1991). World J Surg. 1995; 19:420–422. discussion 423.6. Strodel WE, Eckhauser FE, Lemmer JH, Whitehouse WM Jr, Williams DM. Presentation and perioperative management of arterioportal fistulas. Arch Surg. 1987; 122:563–571.7. Chen Q, Tack C, Morcos M, Ruggiero M, Schlossberg P, Fogel J, et al. Embolotherapy of an arterioportal fistula. Cardiovasc Intervent Radiol. 2007; 30:1047–1051.8. Applbaum YN, Renner JW. Steel coil embolization of hepatoportal fistulae. Cardiovasc Intervent Radiol. 1987; 10:75–79.9. Orons PD, Zajko AB, Jungrels CA. Arterioportal fistula causing portal hypertension and variceal bleeding: treatment with a detachable balloon. J Vasc Interv Radiol. 1994; 5:373–376.10. Pollak JS, White RI Jr. The use of cyanoacrylate adhesives in peripheral embolization. J Vasc Interv Radiol. 2001; 12:907–913.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Gallbladder Fistula Treated with N-Butyl-2-Cyanoacrylate after Radiofrequency Ablation in a Hepatocellular Carcinoma Patient: a Case Report
- Abscesso-Colonic Fistula Following Radiofrequency Ablation Therapy for Hepatocellular Carcinoma; A Case Successfully Treated with Histoacryl Embolization
- Embolization of Seve re Arterioportal Shunts in the Patients with Hepatocellular Carcinoma: Safety and Influence on Patient Survival
- Intrahepatic Arterioportal Shunt:A Mechanism of Hypovascular Hepatocellular Carcinoma
- Multiple Cerebral Infarction after Injection of N-Butyl-2-Cyanoacrylate for Gastric Variceal Bleeding
