Arch Hand Microsurg.
2019 Jun;24(2):197-201. 10.12790/ahm.2019.24.2.197.
Carpal Tunnel Syndrome due to Lipoma: A Case Report
- Affiliations
-
- 1Department of Orthopedic Surgery, Jeju National University School of Medicine, Jeju, Korea. k-mini319@hanmail.net
- KMID: 2448055
- DOI: http://doi.org/10.12790/ahm.2019.24.2.197
Abstract
- Carpal tunnel syndrome is the most common compressive neuropathy in the hand. Median nerve is chronically compressed in a narrow space composed of transverse carpal ligament and carpal bones, which can cause pain, numbness, hypesthesia, and atrophy of the thenar muscle. In most cases, specific causes or factors can not be identified. But space occupied lesions may be locally compressed, or caused by systemic causes such as diabetes and hypothyroidism. Tumors are rarely the cause of local compression in the carpal tunnel. Lipoma is one of the most common soft tissue tumors, but it rarely occurs in the hand, and carpal tunnel syndrome due to compression of lipomas is rarely reported. We report a case of a 65-year-old patient with a diagnosis of carpal tunnel syndrome due to lipoma.
MeSH Terms
Figure
-
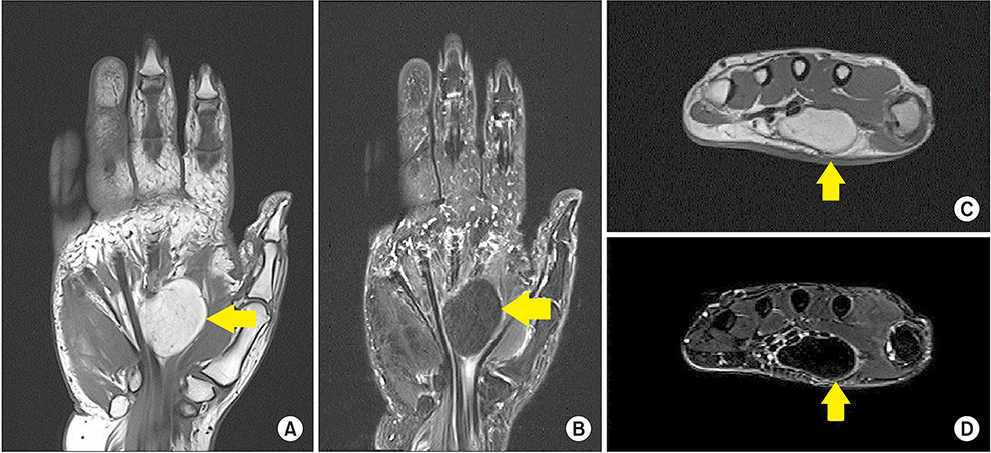
Fig. 1 Magnetic resonance images (A, B) coronal plane T1 weighted image and T2 weighted image (C, D) axial plane T1 weighted image and T2 weighted image. Lipoma is high signal intensity in T1 weighted image and low signal intensity in T2 weighted image.
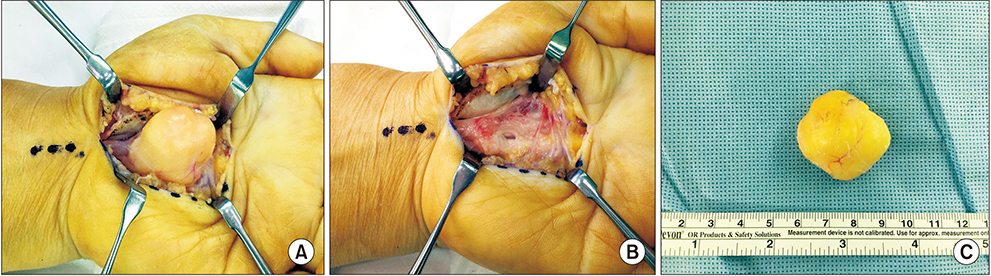
Fig. 2 (A) Intra-operative view of the the median nerve and adherent mass were identified. (B) After a total excision of the mass with epineurolysis and bleeding control. (C) Biopsy specimens, encapsulated and regular margins.
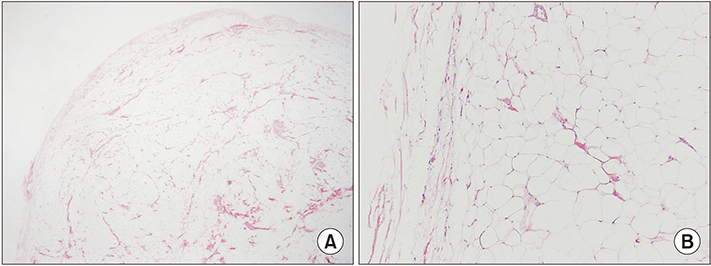
Fig. 3 Microphotographs showing (A) a well-encapsulated adipose tissue mass (H&E stain, ×10), (B) composed of benign mature adipocytes (H&E stain, ×100).
Reference
-
1. de Krom MC, Kester AD, Knipschild PG, Spaans F. Risk factors for carpal tunnel syndrome. Am J Epidemiol. 1990; 132:1102–1110.
Article2. Chen CH, Wu T, Sun JS, Lin WH, Chen CY. Unusual causes of carpal tunnel syndrome: space occupying lesions. J Hand Surg Eur Vol. 2012; 37:14–19.
Article3. Rydholm A, Berg NO. Size, site and clinical incidence of lipoma. Factors in the differential diagnosis of lipoma and sarcoma. Acta Orthop Scand. 1983; 54:929–934.4. Myhre-Jensen O. A consecutive 7-year series of 1331 benign soft tissue tumours. Clinicopathologic data. Comparison with sarcomas. Acta Orthop Scand. 1981; 52:287–293.5. Higgs PE, Young VL, Schuster R, Weeks PM. Giant lipomas of the hand and forearm. South Med J. 1993; 86:887–890.
Article6. Bagatur AE, Zorer G. The carpal tunnel syndrome is a bilateral disorder. J Bone Joint Surg Br. 2001; 83:655–658.
Article7. Nakamichi K, Tachibana S. Unilateral carpal tunnel syndrome and space-occupying lesions. J Hand Surg Br. 1993; 18:748–749.
Article8. Kang HJ, Jung SH, Yoon HK, Hahn SB, Kim SJ. Carpal tunnel syndrome caused by space occupying lesions. Yonsei Med J. 2009; 50:257–261.
Article9. Goodwin RW, O'Donnell P, Saifuddin A. MRI appearances of common benign soft-tissue tumours. Clin Radiol. 2007; 62:843–853.
Article10. McDonagh C, Alexander M, Kane D. The role of ultrasound in the diagnosis and management of carpal tunnel syndrome: a new paradigm. Rheumatology (Oxford). 2015; 54:9–19.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Deep-Seated Giant Lipoma on the Hand Inducing Carpal Tunnel Syndrome
- Ultrasound-Guided Nerve Hydrodissection for Carpal Tunnel Syndrome
- Carpal Tunnel Syndrome in Children with Hypogammaglobulinemia: Case Report
- Extraskeletal Chondroma Causing Carpal Tunnel Syndrome: A Case Report
- An Unusual Cause of Carpal Tunnel Syndrome: A Case of Tuberculosis of the Median Nerve
