First Characterization with Ultrasound Contrast Agent of a Fibrovascular Polyp Before Its Endoscopic Resection: A Case Report (with Videos)
- Affiliations
-
- 1Department of Hepatogastroenterology, University Hospital of Saint-Etienne, Saint-Priest en Jarez, France. nwilliet@yahoo.fr
- 2Department of General Surgery, University Hospital of Saint-Etienne, Saint-Priest en Jarez, France.
- 3Department of Pathology, University Hospital of Saint-Etienne, Saint-Priest en Jarez, France.
- KMID: 2447677
- DOI: http://doi.org/10.5946/ce.2018.083
Abstract
- We described for the first time the contrast enhancement of a giant fibrovascular esophageal polyp using ultrasound contrast agent, Sonovue® (Bracco, Milan, Italy) during echoendoscopy. Fine Doppler was unsuccessful in showing vascularization due to the mobile characteristic of the tumor. In contrast, via Sonovue®, tissue microcirculation was highlighted inside the entire head of the polyp, leading to better appreciate the risk of bleeding related to its resection. In a second part, we showed the feasibility of classic polypectomy for this giant polyp (5×5 cm) without complication and results of control endoscopy at 3 months. The present case is summarized in a video.
Keyword
Figure
-

Fig. 1. Positron emission tomography scanning incidentally showing a non-local glucose metabolic esophageal tumor extended from the cervical esophageal— mouth to the lower esophageal area.
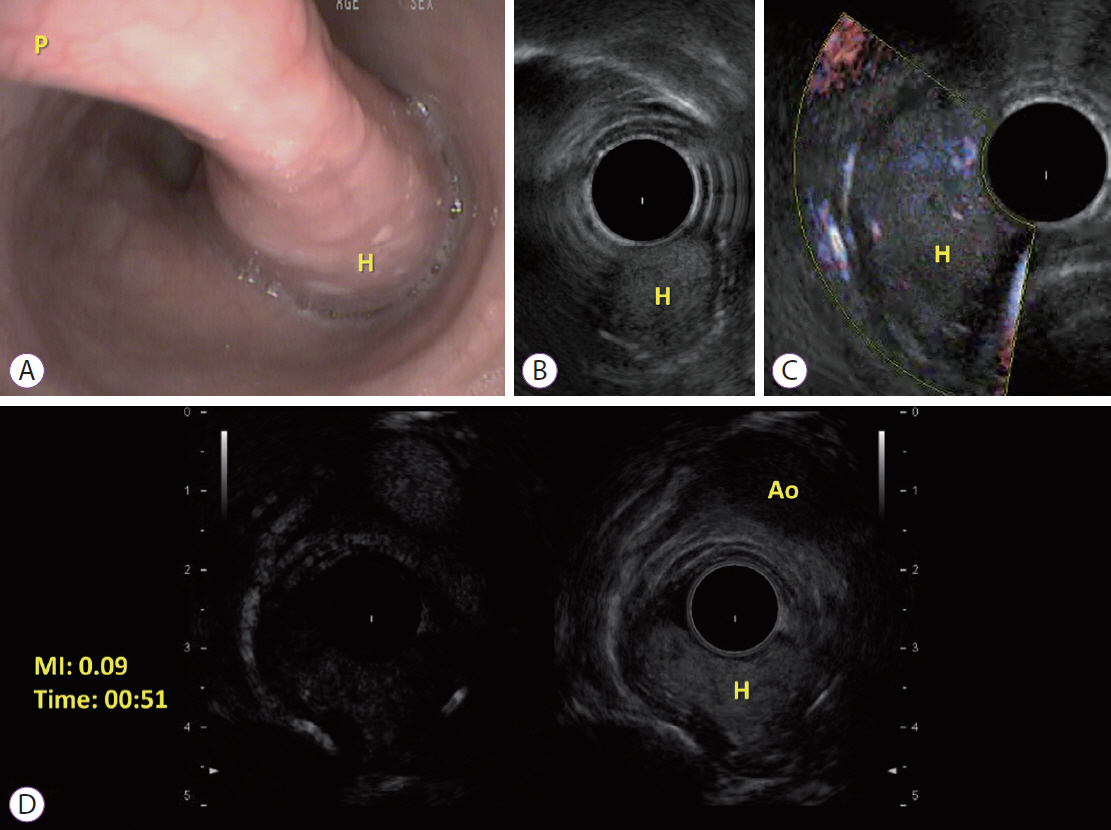
Fig. 2. (A) Endoscopic view of the esophageal fibrovascular polyp. Long thin peduncle (P) and the head (H) of the polyp; (B) Ultrasound endoscopy imaging of the head (H) of the polyp; (C) Idem B with Fine doppler; (D) Contrast-enhanced endoscopic ultrasound of the head (H) of the polyp at the same plane of the aorta (Ao), with low mechanical index (MI).
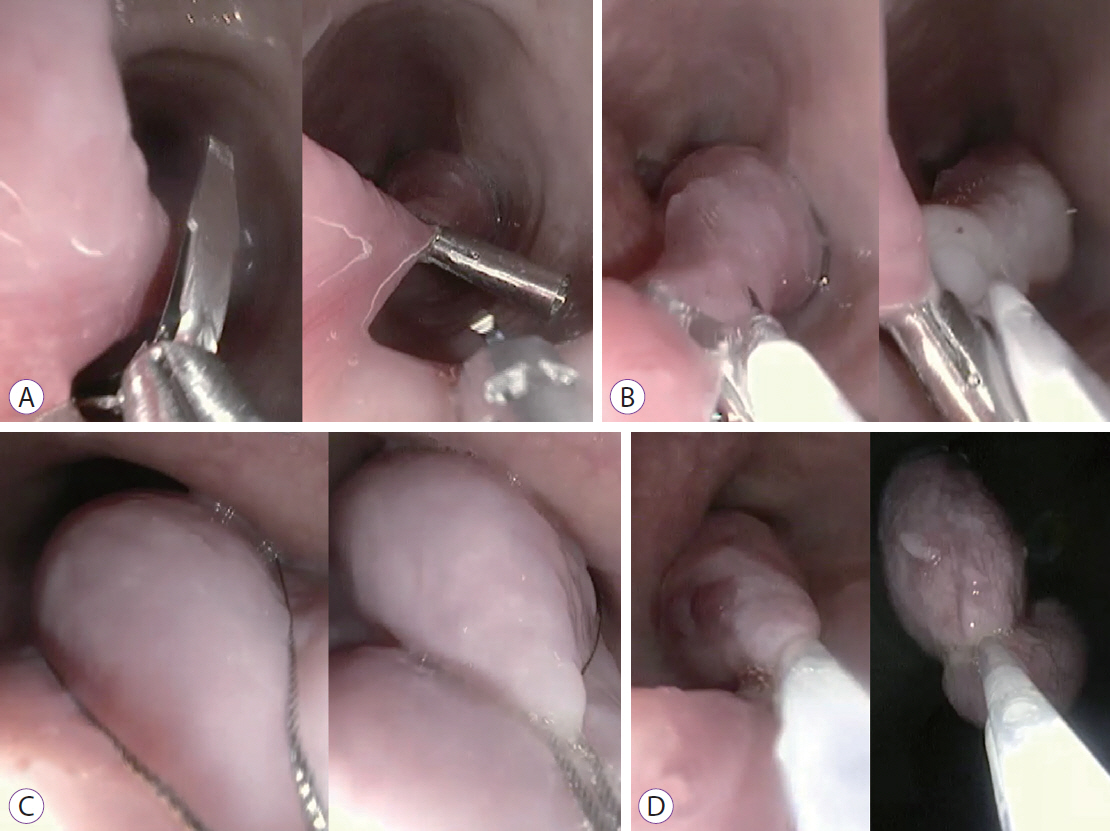
Fig. 3. Steps of fibrovascular polyp resection. (A) Applying a large clip; (B) adrenaline injection; (C) polyp catching with a 30-mm snare; (D) Peduncle coagulation by snare before cutting.
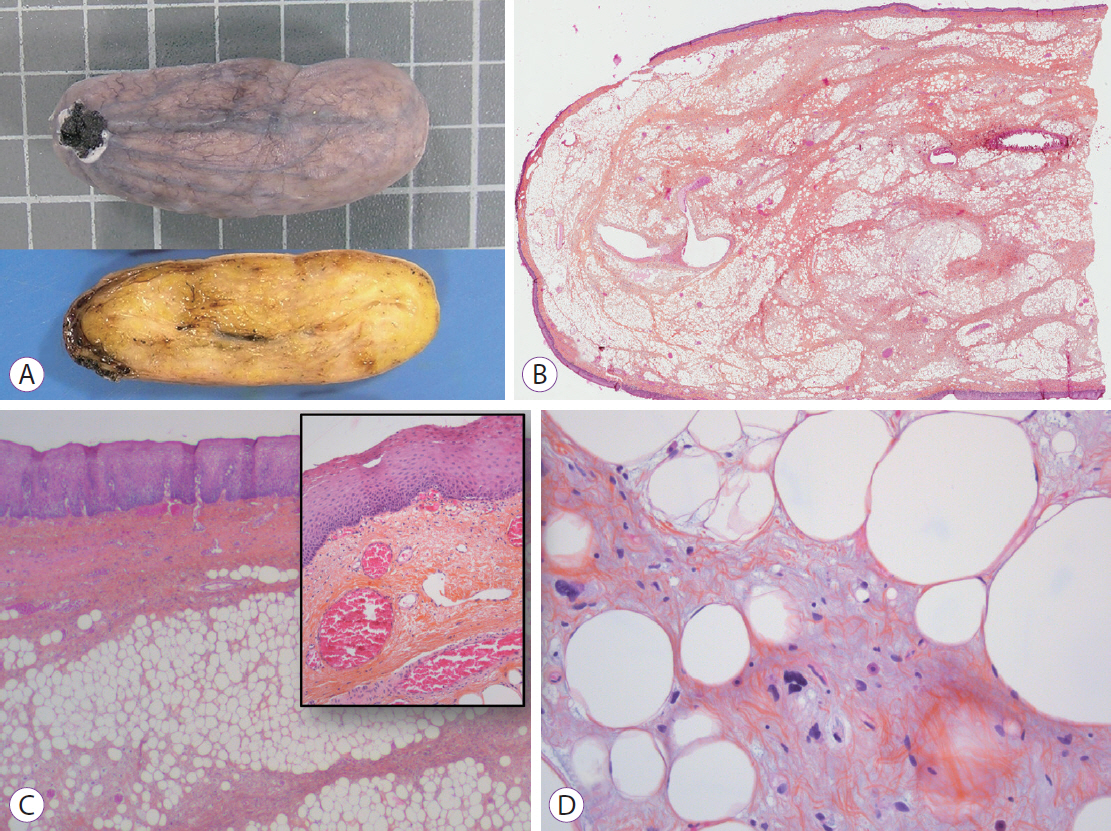
Fig. 4. (A) Upper: gross external aspect (square=1 cm), Lower: cut surface showing homogeneous yellowish color. (B) Low magnification view showing a central fibrous and adipose core surrounded by squamous epithelium, hematoxylin and eosin (H&E), ×1. (C) Squamous epithelium covering the entire surface with dilated vessels below the epithelium, H&E, ×100 (inlay, H&E, ×200). (D) Degenerative atypias of adipocytes, H&E, ×400.
Reference
-
1. Kitano M, Kudo M, Yamao K, et al. Characterization of small solid tumors in the pancreas: the value of contrast-enhanced harmonic endoscopic ultrasonography. Am J Gastroenterol. 2012; 107:303–310.
Article2. Fusaroli P, Spada A, Mancino MG, Caletti G, et al. Contrast harmonic echo-endoscopic ultrasound improves accuracy in diagnosis of solid pancreatic masses. Clin Gastroenterol Hepatol. 2010; 8:629–634. e1-e2.
Article3. Fusaroli P, Eloubeidi MA. Diagnosis of pancreatic cancer by contrast-harmonic endoscopic ultrasound (EUS): complementary and not competitive with EUS-guided fine-needle aspiration. Endoscopy. 2014; 46:380–381.
Article4. Gincul R, Palazzo M, Pujol B, et al. Contrast-harmonic endoscopic ultrasound for the diagnosis of pancreatic adenocarcinoma: a prospective multicenter trial. Endoscopy. 2014; 46:373–379.
Article5. Claudon M, Cosgrove D, Albrecht T, et al. Guidelines and good clinical practice recommendations for contrast enhanced ultrasound (CEUS) - update 2008. Ultraschall Med. 2008; 29:28–44.
Article6. Kannengiesser K, Mahlke R, Petersen F, et al. Contrast-enhanced harmonic endoscopic ultrasound is able to discriminate benign submucosal lesions from gastrointestinal stromal tumors. Scand J Gastroenterol. 2012; 47:1515–1520.
Article7. Fusaroli P, Kypraios D, Mancino MG, et al. Interobserver agreement in contrast harmonic endoscopic ultrasound. J Gastroenterol Hepatol. 2012; 27:1063–1069.
Article8. Park JS, Bang BW, Shin J, et al. A case of esophageal fibrovascular polyp that induced asphyxia during sleep. Clin Endosc. 2014; 47:101–103.
Article9. Lee SY, Chan WH, Sivanandan R, Lim DT, Wong WK. Recurrent giant fibrovascular polyp of the esophagus. World J Gastroenterol. 2009; 15:3697–3700.
Article10. Lorenzo D, Gonzalez JM, Barthet M. Endoscopic resection of a giant esophageal fibrovascular polyp. Endoscopy. 2016; 48 Suppl 1 UCTN:E69–E70.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Giant Fibrovascular Polyp of the Esophagus, Treated Successfully by Endoscopic Resection
- A Case of Fibrovascular Polyp in the Esophagus
- A Case of Large Fibrovascular Polyp of the Stomach
- Less invasive transoral resection of esophageal fibrovascular polyps: case reports
- A Case of Giant Fibrovascular Polyp of the Hypopharynx Removed by Transoral Approach
