Thoracic Outlet Syndrome Induced by Huge Lipoma: A Case Report
- Affiliations
-
- 1Department of Neurosurgery, School of Medicine, Chungnam National University Hospital, Daejeon, Korea. jeongwook.lim@gmail.com
- 2Department of Thoracic and Cardiovascular Surgery, School of Medicine, Chungnam National University Hospital, Daejeon, Korea.
- KMID: 2444209
- DOI: http://doi.org/10.13004/kjnt.2019.15.e9
Abstract
- Thoracic outlet syndrome is a relatively well known disease. Other than trauma, this disease is mostly caused by anatomical structures that cause vascular or neural compression. The cause of thoracic outlet syndrome is diverse; however, there are only few reports of thoracic outlet syndrome caused by lipoma in the pectoralis minor space. We report a case of compression of the lower trunk of brachial plexus in which a large lipoma that developed in the pectoral minor space grew into the subclavicular space, along with a review of literature.
Figure
-
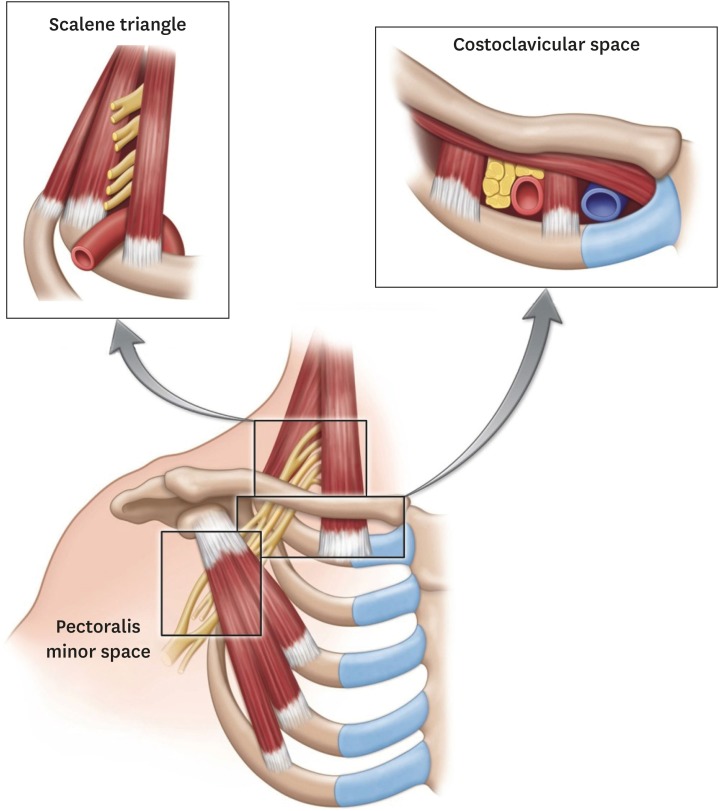
FIGURE 1 Illustration of the thoracic outlet region where thoracic outlet syndrome can occur. Permission was obtained from Wiley Online Library for reprinting this image.
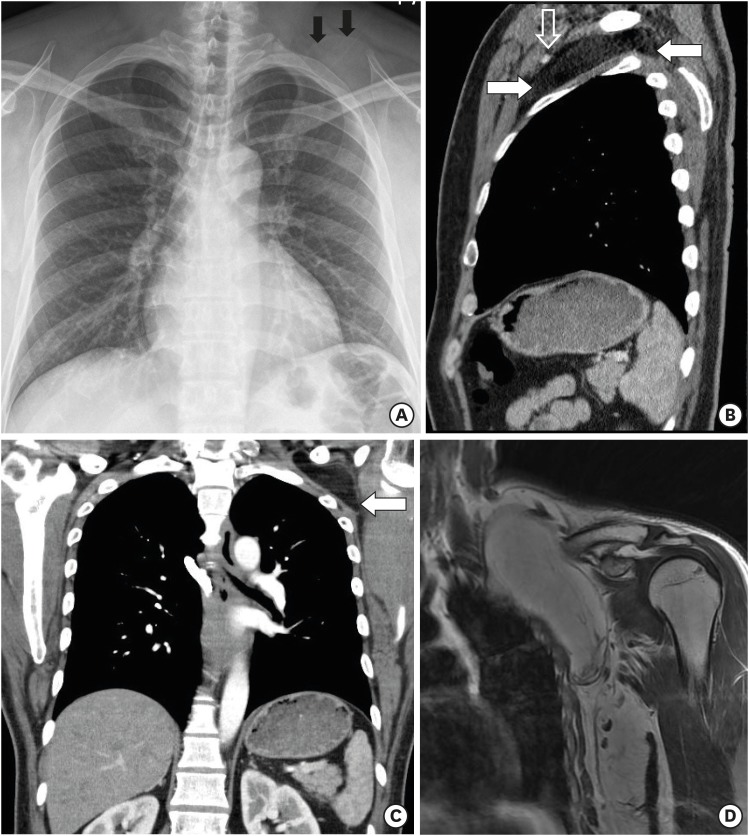
FIGURE 2 (A) Simple chest radiography showing a round mass (black arrow) in the left side upper thorax area. (B, C) Chest computed tomography showing a low density of mass between pectoralis minor space and costoclavicular space, deviated upward direction of vascular bundle (white arrow: mass, open white arrow: neurovascular bundle). (D) Magnetic resonance images of the shoulder showing a huge lipoma in the pectoralis minor space and costoclavicular space.
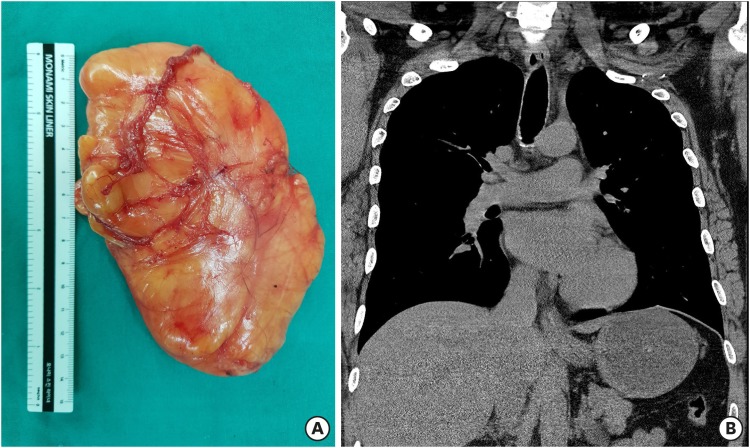
FIGURE 3 (A) Gross photography of the yellowish mass, which was about 0.14 meter. (B) The mass is absent in postoperative chest computed tomography.
Reference
-
1. Demondion X, Boutry N, Drizenko A, Paul C, Francke JP, Cotten A. Thoracic outlet: anatomic correlation with MR imaging. AJR Am J Roentgenol. 2000; 175:417–422. PMID: 10915686.2. Elia S, Cerioli A, Fiaschetti V, Granai AV. Infraclavicular subpectoral lipoma causing thoracic outlet syndrome. Int J Surg Case Rep. 2015; 9:101–104. PMID: 25746951.
Article3. Hussain J, AlZamel HA, Nawaz I, Al Bader A. A case of large deep fibrolipoma in the left subclavicular region that compromised the branchial plexus and thoracic duct: a case report. Int J Surg Case Rep. 2018; 48:139–141. PMID: 29933231.
Article4. Klaassen Z, Sorenson E, Tubbs RS, Arya R, Meloy P, Shah R, et al. Thoracic outlet syndrome: a neurological and vascular disorder. Clin Anat. 2014; 27:724–732. PMID: 23716186.
Article5. Kuyumdzhiev S, Wall ML, Rogoveanu R, Power D, Vohra R. Brachial plexus lipomata presenting with neurogenic and venous thoracic outlet syndrome: case reports and review of the literature. Ann Vasc Surg. 2014; 28:1797.e7–1797.e10.
Article
