J Rheum Dis.
2019 Apr;26(2):124-130. 10.4078/jrd.2019.26.2.124.
Relationship between Urate Crystal Deposits Detected by Dual-energy Computed Tomography and Bone Erosions in Symptomatic Gout Patients without Clinically Apparent Tophi
- Affiliations
-
- 1Division of Rheumatology, Department of Internal Medicine, Ewha Womans University School of Medicine, Seoul, Korea. leejisoo@ewha.ac.kr
- 2Department of Radiology, Ewha Womans University School of Medicine, Seoul, Korea. mshjy@ewha.ac.kr
- KMID: 2442023
- DOI: http://doi.org/10.4078/jrd.2019.26.2.124
Abstract
OBJECTIVE
Dual-energy computed tomography (DECT) allows sensitive detection of monosodium urate (MSU) crystal deposits in gout. However, the role of MSU deposits on DECT during the disease process of gout is not clear. The aim of our study was to evaluate the relationship between joint damage and MSU deposits detected by DECT in symptomatic non-tophaceous gout.
METHODS
DECT scans of 51 gout patients without clinically apparent tophi were assessed. Individual ankle and foot joints and Achilles tendon insertion sites were evaluated for the presence of MSU deposits and bone erosions. The total volume of MSU crystal on DECT was quantified using an automated software program. Clinical and laboratory data at the time of the DECT evaluation were obtained from medical record.
RESULTS
MSU deposits were detected in 92.2% of the patients evaluated. Median number and total volume of MSU deposit per patient was 5.0 and 0.6 cm3, respectively. Bone erosion was found in 54.9% of patients. MSU deposits in the first (1st) metatarsophalangeal (MTP) joints were significantly associated with presence of bone erosions (odds ratio [OR] 3.77, 95% confidence interval [CI] 1.06~13.38, p=0.040). Older age and frequent gout attack were associated with development of bone erosion in patients with MSU deposits (OR 1.12 and 2.57, 95% CI 1.04~1.22 and 1.02~6.50, p-value 0.004 and 0.047, respectively).
CONCLUSION
MSU deposits and erosions were frequently detected by DECT in symptomatic non-tophaceous gout patients, and MSU deposits in 1st MTP joints were associated with presence of bone erosions especially in patients with older age and frequent gout attack.
Figure
-
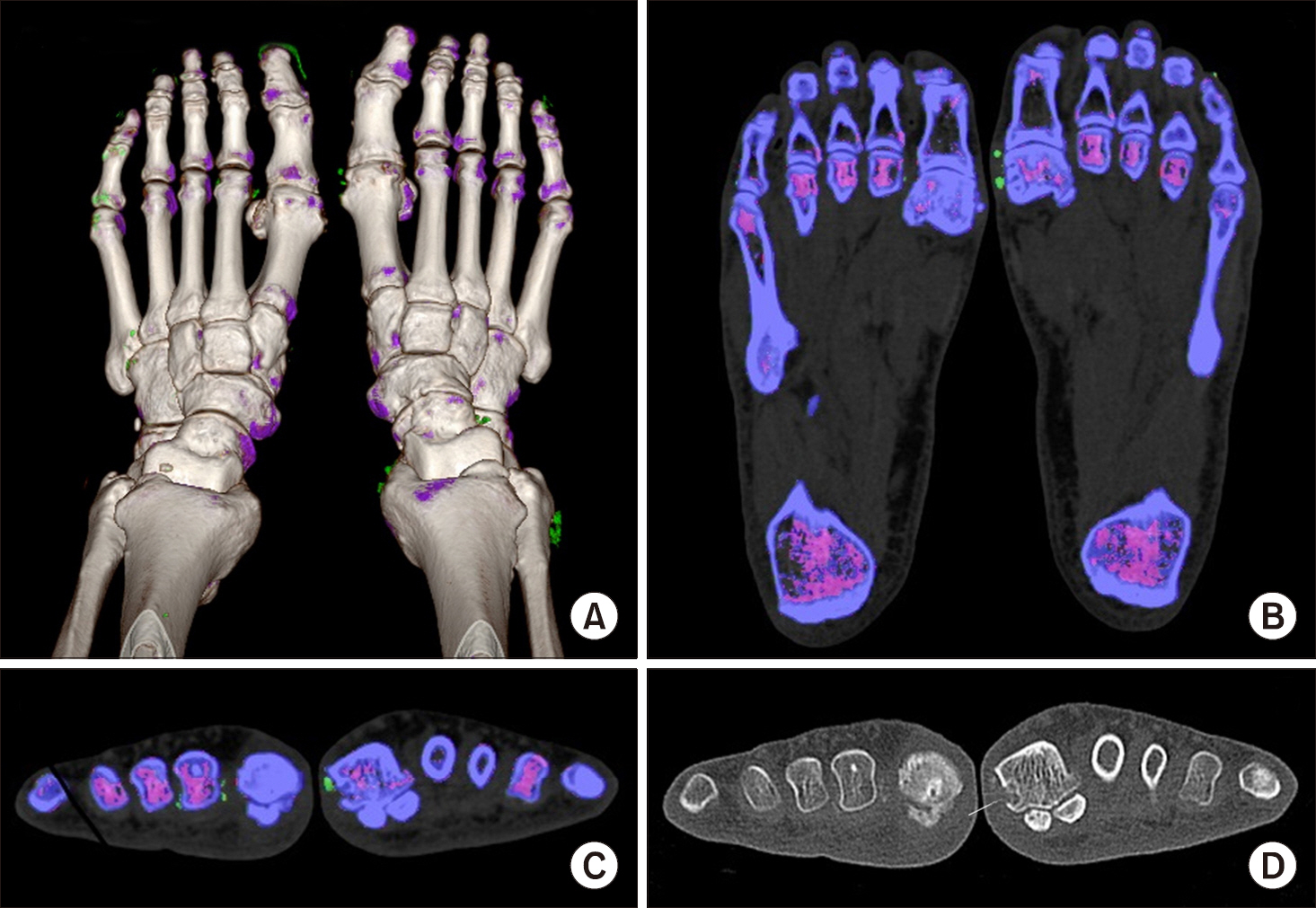
Figure 1. DECT of a 59-year old man with gout. Three-dimensional VRT image of both feet shows green MSU deposits adjacent right first MTP and left second MTP joints (A). Axial DECT image of both feet with small green microtophi (B). Coronal MPR DECT image presenting green microtophi around right first and left second MTP (C). Coronal MPR multi-de-tector CT image which shows erosion on right first MTP (arrow) (D). DECT: dual-energy computed tomography, VRT: volume rendering technique, MSU: monosodium urate, MTP: meta-tarsophalangeal, MPR: multi-planar reformation.
Reference
-
1. Richette P, Bardin T. Gout. Lancet. 2010; 375:318–28.
Article2. Popp JD, Bidgood WD Jr, Edwards NL. Magnetic resonance imaging of tophaceous gout in the hands and wrists. Semin Arthritis Rheum. 1996; 25:282–9.3. McQueen FM, Doyle A, Dalbeth N. Imaging in gout–what can we learn from MRI, CT, DECT and US? Arthritis Res Ther. 2011; 13:246.4. Perez-Ruiz F, Martin I, Canteli B. Ultrasonographic measurement of tophi as an outcome measure for chronic gout. J Rheumatol. 2007; 34:1888–93.5. Thiele RG, Schlesinger N. Diagnosis of gout by ultrasound. Rheumatology (Oxford). 2007; 46:1116–21.
Article6. Bongartz T, Glazebrook KN, Kavros SJ, Murthy NS, Merry SP, Franz WB 3rd, et al. Dual-energy CT for the diagnosis of gout: an accuracy and diagnostic yield study. Ann Rheum Dis. 2015; 74:1072–7.
Article7. Desai MA, Peterson JJ, Garner HW, Kransdorf MJ. Clinical utility of dual-energy CT for evaluation of tophaceous gout. Radiographics. 2011; 31:1365–75.
Article8. Breuer GS, Bogot N, Nesher G. Dual-energy computed tomography as a diagnostic tool for gout during intercritical periods. Int J Rheum Dis. 2016; 19:1337–41.
Article9. Dalbeth N, House ME, Aati O, Tan P, Franklin C, Horne A, et al. Urate crystal deposition in asymptomatic hyperuricaemia and symptomatic gout: a dual energy CT study. Ann Rheum Dis. 2015; 74:908–11.
Article10. Araujo EG, Bayat S, Petsch C, Englbrecht M, Faustini F, Kleyer A, et al. Tophus resolution with pegloticase: a prospective dual-energy CT study. RMD Open. 2015; 1:e000075.
Article11. Dalbeth N, Nicolaou S, Baumgartner S, Hu J, Fung M, Choi HK. Presence of monosodium urate crystal deposition by dual-energy CT in patients with gout treated with allopurinol. Ann Rheum Dis. 2018; 77:364–70.
Article12. Dalbeth N, Aati O, Kalluru R, Gamble GD, Horne A, Doyle AJ, et al. Relationship between structural joint damage and urate deposition in gout: a plain radiography and dual-energy CT study Ann Rheum Dis. 2015; 74:1030–6.13. Choi HK, Al-Arfaj AM, Eftekhari A, Munk PL, Shojania K, Reid G, et al. Dual energy computed tomography in tophaceous gout. Ann Rheum Dis. 2009; 68:1609–12.
Article14. McQueen FM, Doyle A, Reeves Q, Gao A, Tsai A, Gamble GD, et al. Bone erosions in patients with chronic gouty arthropathy are associated with tophi but not bone oedema or synovitis: new insights from a 3 T MRI study. Rheumatology (Oxford). 2014; 53:95–103.
Article15. Dalbeth N, Clark B, Gregory K, Gamble G, Sheehan T, Doyle A, et al. Mechanisms of bone erosion in gout: a quantitative analysis using plain radiography and computed tomography. Ann Rheum Dis. 2009; 68:1290–5.
Article16. Wallace SL, Robinson H, Masi AT, Decker JL, McCarty DJ, Yü TF. Preliminary criteria for the classification of the acute arthritis of primary gout. Arthritis Rheum. 1977; 20:895–900.
Article17. Inker LA, Astor BC, Fox CH, Isakova T, Lash JP, Peralta CA, et al. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am J Kidney Dis. 2014; 63:713–35.
Article18. Mallinson PI, Coupal T, Reisinger C, Chou H, Munk PL, Nicolaou S, et al. Artifacts in dual-energy CT gout protocol: a review of 50 suspected cases with an artifact identification guide. AJR Am J Roentgenol. 2014; 203:W103–9.
Article19. Levin MH, Lichtenstein L, Scott HW. Pathologic changes in gout; survey of eleven necropsied cases. Am J Pathol. 1956; 32:871–95.20. Sokoloff L. The pathology of gout. Metabolism. 1957; 6:230–43.21. McQueen FM, Chhana A, Dalbeth N. Mechanisms of joint damage in gout: evidence from cellular and imaging studies. Nat Rev Rheumatol. 2012; 8:173–81.
Article22. Stewart S, Dalbeth N, Vandal AC, Rome K. The first meta-tarsophalangeal joint in gout: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2016; 17:69.
Article23. Dalbeth N, Merriman TR, Stamp LK. Gout. Lancet. 2016; 388:2039–52.
Article24. Kim SK, Lee H, Kim JH, Park SH, Lee SK, Choe JY. Potential interest of dual-energy computed tomography in gout: focus on anatomical distribution and clinical association. Rheumatology (Oxford). 2013; 52:402–3.
Article25. Sapsford M, Gamble GD, Aati O, Knight J, Horne A, Doyle AJ, et al. Relationship of bone erosion with the urate and soft tissue components of the tophus in gout: a dual energy computed tomography study. Rheumatology (Oxford). 2017; 56:129–33.
Article26. Spaetgens B, van Durme C, Webers C, Tran-Duy A, Schoonbrood T, Boonen A. Construct validity of radiographs of the feet to assess joint damage in patients with gout. J Rheumatol. 2017; 44:91–4.
Article27. Ragab G, Elshahaly M, Bardin T. Gout: an old disease in new perspective – a review. J Adv Res. 2017; 8:495–511.
Article28. Roddy E, Zhang W, Doherty M. Are joints affected by gout also affected by osteoarthritis? Ann Rheum Dis. 2007; 66:1374–7.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ultrasonography and dual-energy computed tomography: impact for the detection of gouty deposits
- Detection of Monosodium Urate Crystal of Hand and Wrist in Suspected Gouty Arthritis Patients on DualEnergy CT and Relationship with Serum Urate Level
- Pathophysiology of Gout
- Chronic Tophaceous Gout of the Calf Mimicking Deep Venous Thrombosis
- Symptomatic Tophaceous Gout in the Bilateral Patellae
