Computerized Tomography is an Effective Modality to Evaluate Iatrogenic Aortocoronary Dissection with Acute Myocardial Infarction
- Affiliations
-
- 1Department of Thoracic and Cardiovascular Surgery, Gil Medical Center, Gachon Cardiovascular Research Institute, Gachon University College of Medicine, Incheon, Korea.
- 2Cardiology Division, Department of Internal Medicine, Gil Medical Center, Gachon Cardiovascular Research Institute, Gachon University College of Medicine, Incheon, Korea. likemed@gilhospital.com
- KMID: 2441141
- DOI: http://doi.org/10.4070/kcj.2018.0284
Abstract
- No abstract available.
MeSH Terms
Figure
-
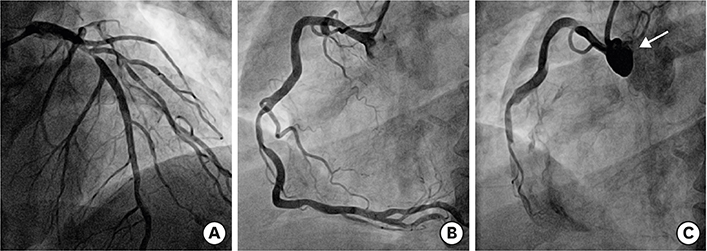
Figure 1 (A, B) Baseline coronary angiogram showed significant stenosis at the proximal left anterior descending artery and the mid RCA. (C) Coronary angiogram showed spiral dissection (arrow) of the RCA from ostium to mid portion with total occlusion. The dissection was extended to the right coronary sinus of the aortic root. RCA = right coronary artery.

Figure 2 Cardiac computerized tomogram. A flap formed by the right coronary artery dissection was identified at the ostium (arrow). Extended dissection flap of aortic root was localized at sinus of Valsalva without propagation into ascending aorta.

Figure 3 (A) Follow-up coronary angiogram on the seventh hospital day showed no interval change of the spiral dissection of RCA. However, localized dissection of sinus of Valsalva was decreased. (B) Percutaneous coronary intervention was performed at the proximal left anterior descending artery with a drug-eluting stent (arrow) and left coronary angiogram showed collateral flow (Rentrop grade 2) from the left coronary artery to the distal RCA (dotted arrow). RCA = right coronary artery.
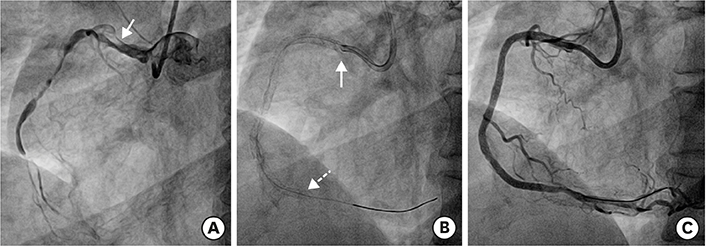
Figure 4 (A) After 3 months, follow-up angiography showed no significant change of the spiral dissection of RCA with slit-like true lumen (arrow). (B) Percutaneous coronary intervention was strugglingly performed from the distal portion (dotted arrow) to the ostium (arrow) of RCA with 4 drug-eluting stents. (C) Completion angiogram showed no visible dissecting flap and no residual stenosis at RCA with thrombolysis in myocardial infarction flow grade 3. RCA = right coronary artery.
Reference
-
1. Dahdouh Z, Roule V, Lognoné T, et al. Iatrogenic bidirectional dissection of the right coronary artery and the ascending aorta: the worst nightmare for an interventional cardiologist. Korean Circ J. 2012; 42:504–506.
Article2. Dunning DW, Kahn JK, Hawkins ET, O'Neill WW. Iatrogenic coronary artery dissections extending into and involving the aortic root. Catheter Cardiovasc Interv. 2000; 51:387–393.
Article3. Li L, Cao Y. Extensive dissection to the coronary sinus of Valsalva during percutaneous intervention in right coronary artery—a case report and literature review. Clin Med Insights Cardiol. 2011; 5:41–44.
Article4. Celik M, Yuksel UC, Yalcinkaya E, Gokoglan Y, Iyisoy A. Conservative treatment of iatrogenic left main coronary artery dissection: report of two cases. Cardiovasc Diagn Ther. 2013; 3:244–246.5. Shorrock D, Michael TT, Patel V, et al. Frequency and outcomes of aortocoronary dissection during percutaneous coronary intervention of chronic total occlusions: a case series and systematic review of the literature. Catheter Cardiovasc Interv. 2014; 84:670–675.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acute Myocardial Infarction in Patient with Spontaneous Coronary
- A Case of Acute Myocardial Infarction Occurred Immediately after Endoscopic Submucosal Dissection
- Invasive Treatment of Acute Myocardial Infarction: What is the Optimal Therapy for Acute Myocardial Infarction?
- A Case of Acute Aortic Dissection Involved Left and Right Coronary Arterial Ostia diagnosed with Transesophageal Echocardiography
- Acute Closure of Target and Remote Coronary Arteries Complicated by Balloon Rupture during Primary Stenting of Acute Myocardial Infarction
