Ann Rehabil Med.
2019 Feb;43(1):38-44. 10.5535/arm.2019.43.1.38.
Does Adequate Lumbar Segmental Motion Reflect Recovery Process in Acute Lumbar Disc Herniation?
- Affiliations
-
- 1Department of Rehabilitation Medicine, Konkuk University School of Medicine & Konkuk University Medical Center, Seoul, Korea. mdlis@kuh.ac.kr
- KMID: 2440950
- DOI: http://doi.org/10.5535/arm.2019.43.1.38
Abstract
OBJECTIVE
To investigate if the extent of lumbar segmental motion is correlated with the recovery process in the form of pain intensity in patients with acute single level lumbar disc herniation (LDH).
METHODS
A retrospective review of medical records was performed on patients presented with acute low back pain from January 2011 to December 2017. With prerequisites of undergoing both lumbar spine magnetic resonance imaging and functional radiography, patients with etiologies other than single level LDH were excluded. A total of 46 patients were selected, including 27 patients with disc herniation at L4-5 level and 19 patients at L5-S1 level. Pearson correlation analysis of pain intensity against segmental range of motion (sROM) and percentage of sROM of each lumbar segment was performed at the initial evaluation point and follow-ups.
RESULTS
Serial documentation of pain intensity and functional radiography exhibited an inverse correlation between changes in visual analogue scale (VAS) and sROM in single level LDH at L4-5 level (r=-0.69, p < 0.05). In addition, percentage of sROM showed a negative correlation with pain intensity at the aforementioned segment (r=-0.74, p < 0.05). Initial pain intensity was also inversely correlated to sROM of the affected segment (r=-0.83, p < 0.01 at L4-5; r=-0.82, p < 0.05 at L5-S1).
CONCLUSION
Improvement in sagittal mobility of the affected segment in LDH adequately reflected mitigation of low back pain during the recovery process. This conjunction could illustrate that the involved segment is overcoming natural immobilization, evidently demonstrating an inverse relationship between initial pain intensity and limitation of sagittal range of motion.
MeSH Terms
Figure
-
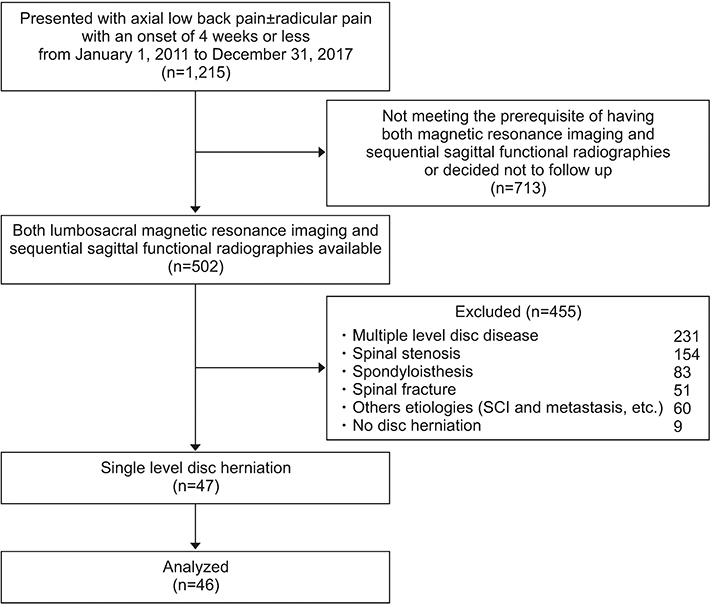
Fig. 1. A diagram depicting the process of patient selection.

Fig. 2. Method of quantifying sagittal range of motion (sROM) of each lumbosacral segment calculated by first measuring the angle between superior and inferior end plates in flexion (A) and extension (B) radiographs and making subtraction at each respective segment. In this particular patient, sROMs of the five lumbosacral segments L1-2, L2-3, L3-4, L4-5, and L5-S1 were determined to be 6°, 9°, 5°, 7°, and 3°, respectively.
Reference
-
1. Vialle LR, Vialle EN, Suarez Henao JE, Giraldo G. Lumbar disc herniation. Rev Bras Ortop. 2015; 45:17–22.
Article2. Jordan J, Konstantinou K, O’Dowd J. Herniated lumbar disc. BMJ Clin Evid. 2009; 2009:1118.3. Katz JN. Lumbar disc disorders and low-back pain: socioeconomic factors and consequences. J Bone Joint Surg Am. 2006; 88 Suppl 2:21–4.
Article4. Malmivaara A, Hakkinen U, Aro T, Heinrichs ML, Koskenniemi L, Kuosma E, et al. The treatment of acute low back pain: bed rest, exercises, or ordinary activity? N Engl J Med. 1995; 332:351–5.5. Szpalski M, Hayez JP. How many days of bed rest for acute low back pain? Objective assessment of trunk function. Eur Spine J. 1992; 1:29–31.
Article6. Dang L, Liu Z. A review of current treatment for lumbar disc herniation in children and adolescents. Eur Spine J. 2010; 19:205–14.
Article7. Atlas SJ, Chang Y, Kammann E, Keller RB, Deyo RA, Singer DE. Long-term disability and return to work among patients who have a herniated lumbar disc: the effect of disability compensation. J Bone Joint Surg Am. 2000; 82:4–15.
Article8. Atlas SJ, Deyo RA. Evaluating and managing acute low back pain in the primary care setting. J Gen Intern Med. 2001; 16:120–31.
Article9. Kim KT, Park SW, Kim YB. Disc height and segmental motion as risk factors for recurrent lumbar disc herniation. Spine (Phila Pa 1976). 2009; 34:2674–8.
Article10. Fardon DF, Williams AL, Dohring EJ, Murtagh FR, Gabriel Rothman SL, Sze GK. Lumbar disc nomenclature: version 2.0: recommendations of the combined task forces of the North American Spine Society, the American Society of Spine Radiology and the American Society of Neuroradiology. Spine J. 2014; 14:2525–45.11. Aspden RM. Intra-abdominal pressure and its role in spinal mechanics. Clin Biomech (Bristol, Avon). 1987; 2:168–74.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Rapid Repeated Recurrent Lumbar Disc Herniation after Microscopic Discectomies
- Lumbar Epidural Venography in the Diagnosis of Lumbar Disc Herniation
- Clinical Analysis of Recurrent Lumbar Disc Herniation
- Juvenile Lumbar Intervertebral Disc Herniation: Five Cases Report
- Lumbar Disc Screening Using Back Pain Questionnaires: Oswestry Low Back Pain Score, Aberdeen Low Back Pain Scale, and Acute Low Back Pain Screening Questionnaire
