Aberrant uterine leiomyomas with extrauterine manifestation: intravenous leiomyomatosis and benign metastasizing leiomyomas
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Institute of Women's Medical Life Science, Yonsei University College of Medicine, Seoul, Korea. ytkchoi@yuhs.ac
- KMID: 2439725
- DOI: http://doi.org/10.5468/ogs.2018.61.4.509
Abstract
OBJECTIVE
Intravenous leiomyomatosis (IVL) and benign metastasizing leiomyoma (BML) are uncommon variants of benign uterine leiomyomas with extrauterine manifestations. Categorizing the extent of disease allows clinicians to delineate the clinical spectrum and the level of sophistication for complete surgical resection.
METHODS
Twelve patients with IVL and BML were reviewed. They were divided into early versus late stage disease groups, and initial manifestation, clinical characteristics, laboratory values, surgical pathology, and follow up data were summarized.
RESULTS
Patients were mostly pre- or peri-menopausal and parous. Patients with late stage disease were more likely to present with cardiac symptoms or abnormal findings on chest X-ray, whereas those with early stage disease presented with classical leiomyoma symptoms including heavy menstrual bleeding, increased myoma size, or lower abdominal discomfort. Tumor marker levels were within normal ranges. A trend of higher neutrophil to leukocyte ratio was observed in the late versus the early stage group (10.4 vs. 1.51, P=0.07); the platelet leukocyte ratio was statistically higher in patients with late stage IVL (0.23 vs. 0.13, P=0.04). The overall recurrence rate was 25%. No recurrence was observed in stage I or stage III IVL groups, while 50% of the stage II IVL group showed recurrence in the pelvic cavity.
CONCLUSION
IVL and BML are benign myoma variants with paradoxically metastatic clinical presentation. Careful inquiry of systemic symptoms, the presence of underlying systemic inflammation, and a high index of suspicion are required for preoperative diagnosis. Furthermore, a multidisciplinary approach is necessary to improve outcomes of surgical resection.
MeSH Terms
Figure
-
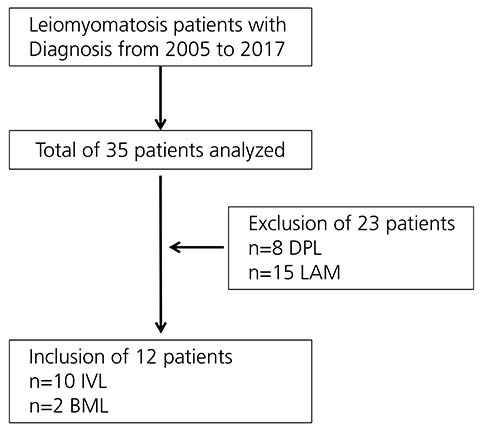
Fig. 1 Flowchart of patient enrollment in the study. DPL, diffuse peritoneal leiomyomatosis; LAM, lymphangioleiomyomatosis; IVL, intravenous leiomyomatosis; BML, benign metastasizing leiomyoma.
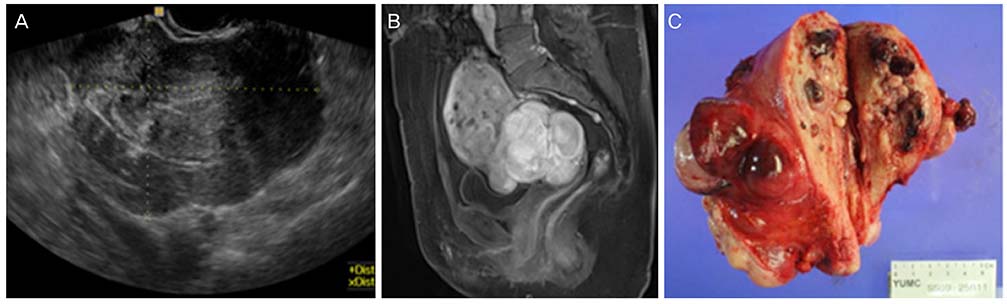
Fig. 2 An example of a stage I, 46-year-old patient with lower abdominal pain. (A) Transvaginal ultrasound showing a conglomeration of multiple intramural myomas and (B) pelvic magnetic resonance imaging showing lobulated subserosal myoma with internal hemorrhage and dilated pelvic vessels. (C) Specimen obtained from total laparoscopic hysterectomy and bilateral salpingo-oophorectomy.
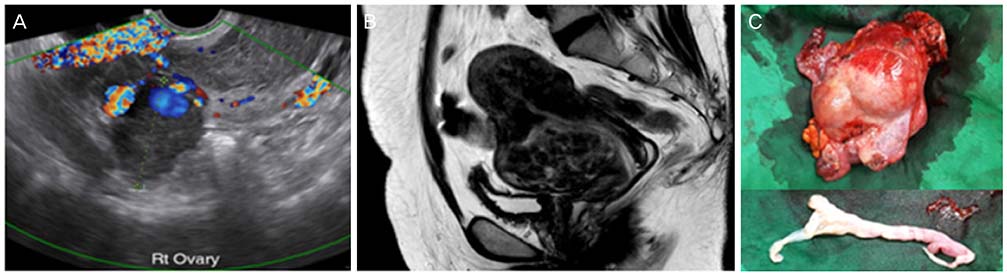
Fig. 3 An example of a stage II, 49-year-old patient with new infiltration of a previously diagnosed myoma on abdomen pelvic computed tomography. (A) Transvaginal ultrasound showing a myoma with extrinsic compression of both adnexa vessels and (B) the pelvic magnetic resonance imaging showing a 9.5 cm myoma with inferior vena cava involvement up to level 3 lumbar vertebra. (C) Specimen obtained from total laparoscopic hysterectomy and bilateral salpingo-oophorectomy, and inferior vena cava mass removal.
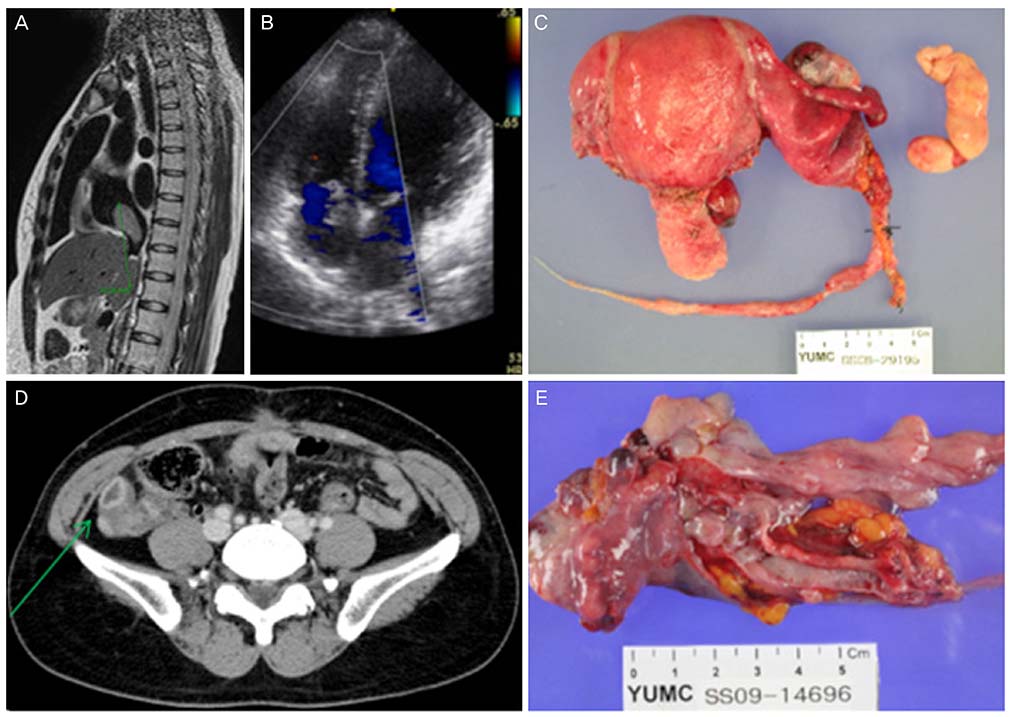
Fig. 4 An example of a stage III, 43-year-old patient presenting with recurrent syncope episode. (A) magnetic resonance imaging showing a 7 cm-sized ‘comma’ shaped thrombosis, extending from the inferior vena cava intrahepatic portion to the right atrium. (B) The transthoracic echocardiography showing an intracardiac mass with dynamic movement past the tricuspid valve into the right ventricle. (C) Specimen from total abdominal hysterectomy, left salpingo-oophorectomy, and inferior vena cava and intracardiac mass removal. (D) One-year follow up showing localized recurrence at right iliac fossa found on abdomen pelvic computed tomography. (E) Specimen obtained from right salpingo-oophorectomy and para-ovarian mass excision.

Fig. 5 An example of a stage IV, 47-year-old patient presenting with heavy menstrual bleeding and history of previous myomectomy. After 3 years of primary surgery total abdominal hysterectomy, bilateral salpingo-oophorectomy, (A) the abdomen pelvic computed tomography showed recurrence with a 12 cm-sized pelvic mass and (B) bilateral lung nodules on chest computed tomography. Specimen obtained from (C) pelvic mass excision and (D) video-assisted thoracoscopic surgery guided resection of bilateral basal lung nodule.
Reference
-
1. Norris HJ, Parmley T. Mesenchymal tumors of the uterus. V. Intravenous leiomyomatosis. A clinical and pathologic study of 14 cases. Cancer. 1975; 36:2164–2178.
Article2. Nam MS, Jeon MJ, Kim YT, Kim JW, Park KH, Hong YS. Pelvic leiomyomatosis with intracaval and intracardiac extension: a case report and review of the literature. Gynecol Oncol. 2003; 89:175–180.
Article3. Solomon LA, Schimp VL, Ali-Fehmi R, Diamond MP, Munkarah AR. Clinical update of smooth muscle tumors of the uterus. J Minim Invasive Gynecol. 2005; 12:401–408.
Article4. Clement PB, Young RH, Scully RE. Intravenous leiomyomatosis of the uterus. A clinicopathological analysis of 16 cases with unusual histologic features. Am J Surg Pathol. 1988; 12:932–945.5. Vaquero ME, Magrina JF, Leslie KO. Uterine smooth-muscle tumors with unusual growth patterns. J Minim Invasive Gynecol. 2009; 16:263–268.
Article6. Patton KT, Cheng L, Papavero V, Blum MG, Yeldandi AV, Adley BP, et al. Benign metastasizing leiomyoma: clonality, telomere length and clinicopathologic analysis. Mod Pathol. 2006; 19:130–140.
Article7. Miller J, Shoni M, Siegert C, Lebenthal A, Godleski J, McNamee C. Benign metastasizing leiomyomas to the lungs: an institutional case series and a review of the recent literature. Ann Thorac Surg. 2016; 101:253–258.
Article8. Lee HJ, Choi J, Kim KR. Pulmonary benign metastasizing leiomyoma associated with intravenous leiomyomatosis of the uterus: clinical behavior and genomic changes supporting a transportation theory. Int J Gynecol Pathol. 2008; 27:340–345.
Article9. Lewis EI, Chason RJ, DeCherney AH, Armstrong A, Elkas J, Venkatesan AM. Novel hormone treatment of benign metastasizing leiomyoma: an analysis of five cases and literature review. Fertil Steril. 2013; 99:2017–2024.
Article10. Ma G, Miao Q, Liu X, Zhang C, Liu J, Zheng Y, et al. Different surgical strategies of patients with intravenous leiomyomatosis. Medicine (Baltimore). 2016; 95:e4902.
Article11. Ordulu Z, Nucci MR, Dal Cin P, Hollowell ML, Otis CN, Hornick JL, et al. Intravenous leiomyomatosis: an unusual intermediate between benign and malignant uterine smooth muscle tumors. Mod Pathol. 2016; 29:500–510.
Article12. Worley MJ Jr, Aelion A, Caputo TA, Kent KC, Salemi A, Krieger KH, et al. Intravenous leiomyomatosis with intracardiac extension: a single-institution experience. Am J Obstet Gynecol. 2009; 201:574.e1–574.e5.
Article13. Cummings M, Merone L, Keeble C, Burland L, Grzelinski M, Sutton K, et al. Preoperative neutrophil:lymphocyte and platelet:lymphocyte ratios predict endometrial cancer survival. Br J Cancer. 2015; 113:311–320.
Article14. Yu X, Zhang G, Lang J, Liu B, Zhao D. Factors associated with recurrence after surgical resection in women with intravenous leiomyomatosis. Obstet Gynecol. 2016; 128:1018–1024.
Article15. Carr RJ, Hui P, Buza N. Intravenous leiomyomatosis revisited: an experience of 14 cases at a single medical center. Int J Gynecol Pathol. 2015; 34:169–176.16. Canzonieri V, D'Amore ES, Bartoloni G, Piazza M, Blandamura S, Carbone A. Leiomyomatosis with vascular invasion. A unified pathogenesis regarding leiomyoma with vascular microinvasion, benign metastasizing leiomyoma and intravenous leiomyomatosis. Virchows Arch. 1994; 425:541–545.
Article17. Bodner-Adler B, Bartl M, Wagner G. Intravenous leiomyomatosis of the uterus with pulmonary metastases or a case with benign metastasizing leiomyoma? Anticancer Res. 2009; 29:495–496.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Leiomyomatosis Peritonealis Disseminata
- Uterine Leiomyomas with Perinodular Hydropic Degeneration: A Report of Two Cases
- Disseminated Peritoneal Leiomyomatosis Following Previous Laparoscopic Myomectomy with Morcellation
- Intravenous Leiomyomatosis with Extension to the Heart Associated with Disseminated Peritoneal Leiomyomatosis
- Diffuse Leiomyomatosis of The Esophagus: A Case Report
