J Korean Orthop Assoc.
2019 Feb;54(1):59-66. 10.4055/jkoa.2019.54.1.59.
Reliable Radiologic Parameters to Predict Surgical Management for Clubfoot Treated with the Ponseti Method
- Affiliations
-
- 1Department of Orthopedic Surgery, Keimyung University School of Medicine, Daegu, Korea. poweryon@nate.com
- KMID: 2438965
- DOI: http://doi.org/10.4055/jkoa.2019.54.1.59
Abstract
- PURPOSE
Several radiologic reference lines have been used to evaluate individuals with a clubfoot but there is no consensus as to which is most reliable. The aim of this study was to identify which radiologic parameters have relevance to the predictability of additional surgery after Ponseti casting on clubfoot and the effect of clubfoot treatments that contain Ponseti casting and additional surgery.
MATERIALS AND METHODS
A total of 102 clubfeet (65 patients, 37 bilateral) were reviewed from 2005 to 2013. The patients were divided into two groups (Group A, those for whom the result of the Ponseti method was successful and did not require additional surgery; and Group B, those for whom the result of the Ponseti method was unsuccessful and required additional surgery), and the following parameters were measured on the plain radiographs: i) talo-calcaneal angle on the anteroposterior and lateral view, ii) talo-1st metatarsal angle on the anteroposterior view, and iii) Tibio-calcaneal angle on the lateral view with the ankle full-dorsiflexion state. Each radiograph was reviewed on two separate occasions by one orthopedic doctor to characterize the intra-observer reliability, and the averages were analyzed. Next, 20 cases were chosen using a random number table, and two orthopedic doctors measured the angle separately to characterize the inter-observer reliability.
RESULTS
Groups A and B included 73 clubfeet (71.6%) and 29 clubfeet (28.4%), respectively. The initial talo-calcaneal angle and tibio-calcaneal angle in the lateral view were significantly different among the groups. In addition, inter- and intra-observer biases were not detected. The talo-1st metatarsal angle on the anteroposterior view and tibio-calcaneal angle on the lateral view were significantly different after treatment in both groups.
CONCLUSION
Congenital clubfeet treated with the Ponseti method showed successful results in more than 70% of patients. The initial talo-calcaneal angle and tibio-calcaneal angle on the lateral view were the radiologic parameters that could predict the need for additional surgical treatments. The talo-1st metatarsal angle on the anteroposterior view and tibio-calcaneal angle on the lateral view could effectively evaluate the changes in clubfoot after treatment.
Keyword
Figure
-
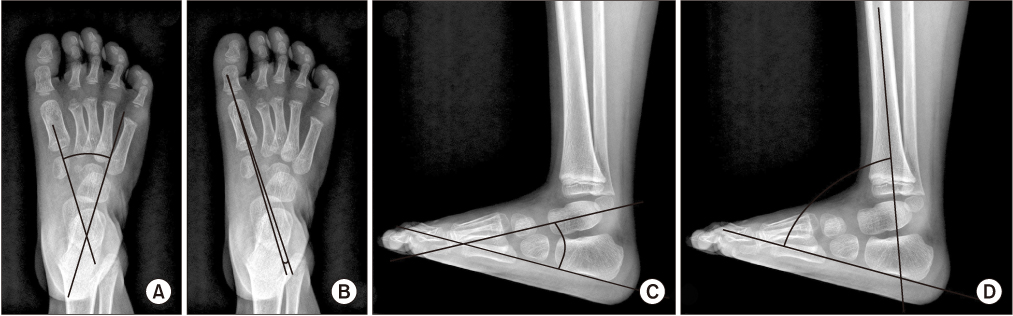
Figure 1 (A) Talo-calcaneal angle on the anteroposterior view. (B) Talo-1st metatarsal angle on the anteroposterior view. (C) Talo-calcaneal angle on the lateral view. (D) Tibio-calcaneal angle on the lateral view.
Reference
-
1. Dobbs MB, Rudzki JR, Purcell DB, Walton T, Porter KR, Gurnett CA. Factors predictive of outcome after use of the Ponseti method for the treatment of idiopathic clubfeet. J Bone Joint Surg Am. 2004; 86:22–27.
Article2. Herzenberg JE, Radler C, Bor N. Ponseti versus traditional methods of casting for idiopathic clubfoot. J Pediatr Orthop. 2002; 22:517–521.
Article3. Cooper DM, Dietz FR. Treatment of idiopathic clubfoot. A thirty-year follow-up note. J Bone Joint Surg Am. 1995; 77:1477–1489.
Article4. Laaveg SJ, Ponseti IV. Long-term results of treatment of congenital club foot. J Bone Joint Surg Am. 1980; 62:23–31.
Article5. Ponseti IV, Smoley EN. The classic: congenital club foot: the results of treatment. 1963. Clin Orthop Relat Res. 2009; 467:1133–1145.6. Radler C, Manner HM, Suda R, et al. Radiographic evaluation of idiopathic clubfeet undergoing Ponseti treatment. J Bone Joint Surg Am. 2007; 89:1177–1183.
Article7. Kite JH. Principles involved in the treatment of congenital club-foot. 1939. J Bone Joint Surg Am. 2003; 85:1847. discussion 1847.8. Kite JH. The clubfoot. New York: Grune & Stratton;1964. p. 232.9. Kite JH. Conservative treatment of the resistant recurrent clubfoot. Clin Orthop Relat Res. 1970; 70:93–110.
Article10. Kite JH. Nonoperative treatment of congenital clubfoot. Clin Orthop Relat Res. 1972; 84:29–38.11. Park SS, Kim SW, Jung BS, Lee HS, Kim JS. Selective soft-tissue release for recurrent or residual deformity after conservative treatment of idiopathic clubfoot. J Bone Joint Surg Br. 2009; 91:1526–1530.
Article12. Ponseti IV. Congenital clubfoot: fundamentals of treatment. Oxford: Oxford University Press;1996. p. 140.13. Simons GW. Analytical radiography of club feet. J Bone Joint Surg Br. 1977; 59:485–489.
Article14. Colburn M, Williams M. Evaluation of the treatment of idiopathic clubfoot by using the Ponseti method. J Foot Ankle Surg. 2003; 42:259–267.
Article15. Frick SL. The Ponseti method of treatment for congenital clubfoot: importance of maximal forefoot supination in initial casting. Orthopedics. 2005; 28:63–65.
Article16. Hamel J, Becker W. Sonographic assessment of clubfoot deformity in young children. J Pediatr Orthop B. 1996; 5:279–286.
Article17. Simons GW. A standardized method for the radiographic evaluation of clubfeet. Clin Orthop Relat Res. 1978; 107–118.
Article18. Shapiro F, Glimcher MJ. Gross and histological abnormalities of the talus in congenital club foot. J Bone Joint Surg Am. 1979; 61:522–530.
Article19. Fritsch H, Eggers R. Ossification of the calcaneus in the normal fetal foot and in clubfoot. J Pediatr Orthop. 1999; 19:22–26.
Article20. Diméglio A, Bonnet F, Mazeau P, De Rosa V. Orthopaedic treatment and passive motion machine: consequences for the surgical treatment of clubfoot. J Pediatr Orthop B. 1996; 5:173–180.21. Thacker MM, Scher DM, Sala DA, van Bosse HJ, Feldman DS, Lehman WB. Use of the foot abduction orthosis following Ponseti casts: is it essential? J Pediatr Orthop. 2005; 25:225–228.22. Shim JS, Seo SW, Kim CY, Jung C. Congenital clubfoot treated with the Ponseti method. J Korean Orthop Assoc. 2009; 44:634–641.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Relapse of Clubfoot after Treatment with the Ponseti Method and the Function of the Foot Abduction Orthosis
- Congenital Clubfoot Treated with the Ponseti Method
- Peroneal Nerve Dysfunction in Patients with Clubfoot Deformity: Evaluation of Clinical Presentation and Treatment
- Results of a Standard versus an Accelerated Ponseti Protocol for Clubfoot: A Prospective Randomized Study
- Results of Surgical Treatment for Congenital Vertical Talus
