Anesth Pain Med.
2018 Jul;13(3):292-297. 10.17085/apm.2018.13.3.292.
Iatrogenic common carotid artery rupture during neck surgery rescued using covered stent: A case report
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Gyeongsang National University Hospital, Jinju, Korea. ilwooshin@gnu.ac.kr
- 2Department of Anesthesiology and Pain Medicine, Gyeongsang National University School of Medicine, Jinju, Korea.
- 3Department of Anesthesiology and Pain Medicine, Institute of Health Sciences, Gyeongsang National University, Jinju, Korea.
- KMID: 2436037
- DOI: http://doi.org/10.17085/apm.2018.13.3.292
Abstract
- Carotid artery rupture during head and neck surgery is a catastrophic, life-threatening emergency. Although recent incidence has declined, it still occurs in many patients. Hemorrhage from the carotid artery is usually massive and uncontrollable. Fast, aggressive treatment to prevent hemodynamic instability is required. Even if patients survive this event, they may experience severe neurological sequelae. A ruptured carotid artery is usually controlled by direct compression and arterial ligation. However, apart from the inherent difficulty of operation, these traditional surgical treatments are associated with high morbidity and mortality. In the past two decades, endovascular management has become a mainstay of carotid rupture treatment. We report a case of successful recovery without any sequelae after cardiovascular collapse due to an unintentional common carotid artery (CCA) rupture during neck surgery. The exposed CCA was treated with a covered stent. In such a case, multidisciplinary cooperation is crucial.
MeSH Terms
Figure
-

Fig. 1 Angiography of a ruptured common carotid artery. The site of rupture is compressed by gauze packing and a hand. This carotid angiography shows a bleeding focus of extravasation and decreased blood flow of the internal and external carotid arteries.

Fig. 2 Covered stent. A covered stent is composed of a special fabric and metal (W. L. Gore and Associates, USA).
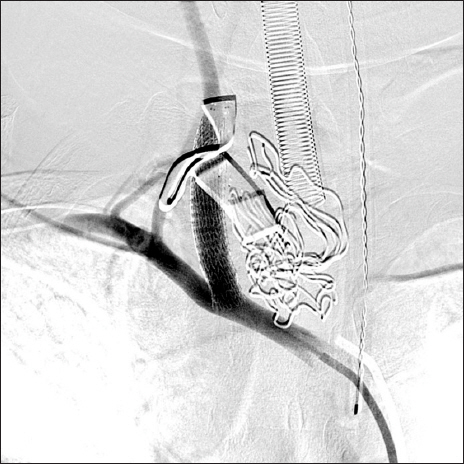
Fig. 3 Ruptured common carotid artery successfully repaired by stent. This carotid angiography demonstrates well-maintained distal flow to the carotid artery and subclavian artery.
Reference
-
1. Iqbal S. A comprehensive study of the anatomical variations of the circle of willis in adult human brains. J Clin Diagn Res. 2013; 7:2423–7. DOI: 10.7860/JCDR/2013/6580.3563.2. Citardi MJ, Chaloupka JC, Son YH, Ariyan S, Sasaki CT. Management of carotid artery rupture by monitored endovascular therapeutic occlusion (1988-1994). Laryngoscope. 1995; 105:1086–92. DOI: 10.1288/00005537-199510000-00015. PMID: 7564841.3. La Vecchia C, Malvezzi M, Bosetti C, Garavello W, Bertuccio P, Levi F, et al. Thyroid cancer mortality and incidence: a global overview. Int J Cancer. 2015; 136:2187–95. DOI: 10.1002/ijc.29251. PMID: 25284703.4. Hamming JF, Roukema JA. Management of regional lymph nodes in papillary, follicular, and medullary thyroid cancer. Textbook of endocrine surgery. 3rd ed. Clark OH, Duh QY, Kebebew E, Gosnell JE, Shen WT, editors. New Delhi: Jaypee Brothers Medical Publishers Ltd;2016. p. 407–8.5. Gómez-Ramírez J, Sitges-Serra A, Moreno-Llorente P, Zambudio AR, Ortega-Serrano J, Rodríguez MT, et al. Mortality after thyroid surgery, insignificant or still an issue? Langenbecks Arch Surg. 2015; 400:517–22. DOI: 10.1007/s00423-015-1303-1. PMID: 25900848.6. Cheah WK, Arici C, Ituarte PH, Siperstein AE, Duh QY, Clark OH. Complications of neck dissection for thyroid cancer. World J Surg. 2002; 26:1013–6. DOI: 10.1007/s00268-002-6670-4. PMID: 12045861.7. Haas RA, Ahn SH. Interventional management of head and neck emergencies: carotid blowout. Semin Intervent Radiol. 2013; 30:245–8. DOI: 10.1055/s-0033-1353477. PMID: 24436546. PMCID: PMC3773042.8. Zealley IA, Chakraverty S. The role of interventional radiology in trauma. BMJ. 2010; 340:c497. DOI: 10.1136/bmj.c497. PMID: 20142319.9. Lesley WS, Chaloupka JC, Weigele JB, Mangla S, Dogar MA. Preliminary experience with endovascular reconstruction for the management of carotid blowout syndrome. AJNR Am J Neuroradiol. 2003; 24:975–81. PMID: 12748106.10. Song JH, Lee HS, Han JU, Jung JK, Kim HZ, Shinn HK. Anesthetic management for liver segmentectomy and thrombectomy of inferior vena cava and right atrium without cardiopulmonary bypass: a case report. Anesth Pain Med. 2007; 2:224–7.11. Fukuda S, Warner DS. Cerebral protection. Br J Anaesth. 2007; 99:10–7. DOI: 10.1093/bja/aem140. PMID: 17573393.12. Dewhurst AT, Moore SJ, Liban JB. Pharmacological agents as cerebral protectants during deep hypothermic circulatory arrest in adult thoracic aortic surgery. A survey of current practice. Anaesthesia. 2002; 57:1016–21. DOI: 10.1046/j.1365-2044.2002.02787.x. PMID: 12358961.13. Zhou J, Lian J, Li HX, Hong GL, Zhao GJ, Zhi SC, et al. [Mechanism research and effect of ulinastatin in the brain tissue injury of acute hydrogen sulfide intoxicated rats]. Chin J Ind Hyg Occup Dis. 2016; 34:166–72.14. Jiang XM, Hu JH, Wang LL, Ma C, Wang X, Liu XL. Effects of ulinastatin on global ischemia via brain pro-inflammation signal. Transl Neurosci. 2016; 7:158–63. DOI: 10.1515/tnsci-2016-0023. PMID: 28123836. PMCID: PMC5234523.15. Demirci M, Saribaş O, Uluç K, Cekirge S, Böke E, Ay H. Carotid artery stenting and endarterectomy have different effects on heart rate variability. J Neurol Sci. 2006; 241:45–51. DOI: 10.1016/j.jns.2005.10.011. PMID: 16325863.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Iatrogenic Subclavian Artery Perforation Rescued by Operator-Modified Graft Stent
- Delayed Rupture of the Carotid artery After Automobile Accident: An Autopsy Case
- Stent-Graft Repair of Common Carotid Pseudoaneurysms in Behcet's Syndrome
- A Case of Spontaneous Hemorrhage of Ruptured Hemangioma Originated from Carotid Artery
- A case of rupture of the common carotid artery by gunshot injury
