Cervical varix with thrombosis diagnosed in the first trimester of pregnancy
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Kyungpook National University Hospital, Kyungpook National University School of Medicine, Daegu, Korea. ties1004@naver.com
- KMID: 2430931
- DOI: http://doi.org/10.5468/ogs.2019.62.1.65
Abstract
- Cervical varix is rare and can develop due to various conditions in pregnancy. Most cases of cervical varix during pregnancy are diagnosed in the second or third trimester and are usually associated with abnormal placental location, such as placenta previa or low-lying placenta. A 23-year-old woman with cervical varix bleeding visited our institution at 8 weeks of gestation. This case report describes cervical varix bleeding that developed into a venous thrombus in the first trimester. Ultrasonography with color Doppler and magnetic resonance imaging could be helpful in diagnosis.
Keyword
MeSH Terms
Figure
-
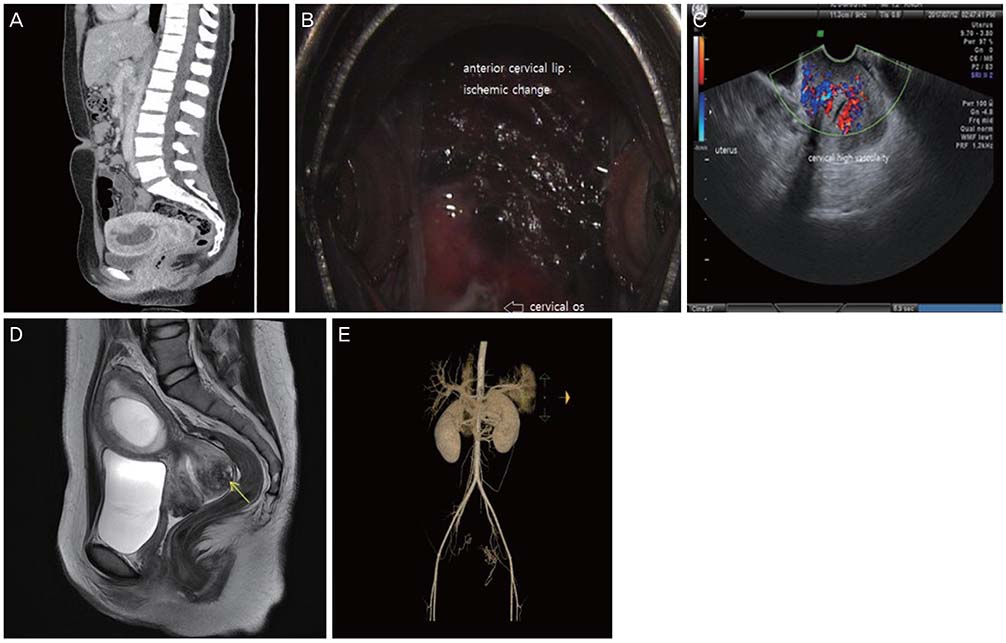
Fig. 1 (A) Computed tomography showed a cervical varix following presentation with high fever. Computed tomography revealed an intrauterine pregnancy with no other cervical abnormality. (B) The bleeding focus and cervical varix with erosion. A dark-red color change was observed in the anterior cervical lip. (C) Transvaginal ultrasonography showed cervical hypervascularity. (D) Magnetic resonance imaging showed diffuse cervical prominence with a dilated vascular channel partially filled with thrombus. (E) Computed tomography angiography showed arterial and venous hypervascularity in the cervix, which was supplied with blood from the internal iliac artery.

Fig. 2 Appearance at the first visit after discharge. (A) Ultrasonography showed that the cervical varix had disappeared. (B) Colposcopy showed normal morphology.
Reference
-
1. Gabbe SG, Niebyl JR, Simpson JL. Obstetrics: normal and problem pregnancy. 4th ed. New York (NY): Elsevier;2002.2. Chapman AB, Abraham WT, Zamudio S, Coffin C, Merouani A, Young D, et al. Temporal relationships between hormonal and hemodynamic changes in early human pregnancy. Kidney Int. 1998; 54:2056–2063.
Article3. Stansby G. Women, pregnancy, and varicose veins. Lancet. 2000; 355:1117–1118.
Article4. Fleming AD, Anderson TL. Cervical AV malformation with in utero DES exposure. Nebr Med J. 1993; 78:138–139.5. Follen MM, Fox HE, Levine RU. Cervical vascular malformation as a cause of antepartum and intrapartum bleeding in three diethylstilbestrol-exposed progeny. Am J Obstet Gynecol. 1985; 153:890–891.
Article6. Sammour RN, Gonen R, Ohel G, Leibovitz Z. Cervical varices complicated by thrombosis in pregnancy. Ultrasound Obstet Gynecol. 2011; 37:614–616.
Article7. Sükür YE, Yalçın I, Kahraman K, Söylemez F. Cervical varix complicating marginal placenta previa: a unique coexistence. J Obstet Gynaecol Res. 2011; 37:1515–1517.8. Kurihara Y, Tachibana D, Teramae M, Matsumoto M, Terada H, Sumi T, et al. Pregnancy complicated by cervical varix and low-lying placenta: a case report. Jpn Clin Med. 2013; 4:21–24.
Article9. Leibovitz Z, Degani S, Shapiro I, Tal J, Paz B, Levitan Z, et al. Diagnosis of pregnancy-associated uterine venous plexus thrombosis on the basis of transvaginal sonography. J Ultrasound Med. 2003; 22:287–293.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Radiologic Findings of Cervical Varix Developed in Late Pregnancy: Case Report
- A Case Report of Cervical Prolapse Complicating Pregnancy
- Cevix Cancer Associated with Pregnancy: A Case Report and Review of the Literature
- Fetal Wastage in the Second-Trimester of Pregnancy: An Obstetric Approach
- Placenta Increta Presenting as Postabortal Uterine Mass in the First Trimester: A Case Report
