Right Atrial Deformation Mechanics in Children with Adenotonsillar Hypertrophy
- Affiliations
-
- 1Department of Pediatrics, CHA Bundang Medical Center, CHA University School of Medicine, Seongnam, Korea. kittysooni@chamc.co.kr
- KMID: 2429994
- DOI: http://doi.org/10.4250/jcvi.2018.26.e26
Abstract
- BACKGROUND
Children with significant adenotonsillar hypertrophy (ATH) may show right ventricular (RV) dysfunction. We aimed to evaluate RV dysfunction in such children before adenotonsillectomy by evaluating peak longitudinal right atrial (RA) strain (PLRAS) in systole. PLRAS, electrocardiogram (ECG) and conventional echocardiographic parameters were compared to distinguish children with significant ATH with sleep-related breathing disorder (ATH-SRBD) from controls.
METHODS
Fifty-six children (23 controls and 33 children with ATH-SRBD without symptoms of heart failure) were retrospectively studied. Preoperative echocardiograms and ECGs of children with ATH-SRBD who underwent adenotonsillectomy were compared to those of controls. Available postoperative ECGs and echocardiograms were also analyzed.
RESULTS
Preoperatively, prolonged maximum P-wave duration (Pmax) and P-wave dispersion (PWD), decreased PLRAS, and increased tricuspid annulus E/E"² were found in children with ATH-SRBD compared to those of controls. From the receiver operating characteristic curves, PLRAS was not inferior compared to tricuspid annulus E/E"², Pmax, and PWD in differentiating children with ATH-SRBD from controls; however, the discriminative abilities of all four parameters were poor. In children who underwent adenotonsillectomy, echocardiograms 1.2 ± 0.4 years after adenotonsillectomy showed no difference in postoperative PLRAS and tricuspid annulus E/E"² when compared with those of the preoperative period.
CONCLUSIONS
Impaired RA deformation was reflected as decreased PLRAS in children with ATH-SRBD before adenotonsillectomy. Decreased PLRAS in these children may indicate subtle RV dysfunction and increased proarrhythmic risk. However, usefulness of PLRAS as an individual parameter in differentiating preoperative children with ATH-SRBD from controls was limited, similar to those of tricuspid annulus E/E"², Pmax, and PWD.
Keyword
MeSH Terms
Figure
-

Figure 1 A velocity vector imaging of peak longitudinal right atrial strain during systole. RA: right atrium.

Figure 2 An example of PLRAS during systole obtained as the average of the three segments of the right atrium (septum, lateral wall, and roof) from a healthy control. PLRAS: peak longitudinal right atrial strain.

Figure 3 An example of PLRAS during systole obtained as the average of the three segments of the right atrium (septum, lateral wall, and roof) preoperatively from a child with significant adenotonsillar hypertrophy and sleep-related breathing disorder. PLRAS: peak longitudinal right atrial strain.

Figure 4 Comparison of PLRAS during systole and tricuspid annulus E/E′ between controls and preoperative children with ATH-SRBD. ATH-SRBD: significant adenotonsillar hypertrophy and sleep-related breathing disorder. E/E′: the ratio between tricuspid inflow Doppler velocity during early diastole (E) and tricuspid annular tissue Doppler velocity during early diastole (E′), PLRAS: peak longitudinal right atrial strain. Blue boxes represent controls, green boxes represent children with ATH-SRBD. *p < 0.05 when compared with controls.
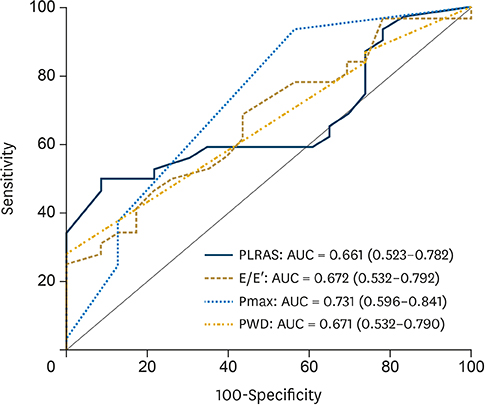
Figure 5 Receiver operating characteristic curves of PLRAS during systole, tricuspid annulus E/E′, and electrocardiographic parameters (Pmax and PWD) to differentiate children with significant adenotonsillar hypertrophy and sleep-related breathing disorder from controls. AUC: area under the curve, E/E′: tricuspid inflow Doppler velocity during early diastole (E) and tricuspid annular tissue Doppler velocity during early diastole (E′), PLRAS: peak right atrial longitudinal strain, Pmax: maximum P-wave duration, PWD: P-wave dispersion. The numbers in parentheses represent the 95% confidence intervals for the AUCs. The p values (area = 0.5) for AUCs of PLRAS, tricuspid annulus E/E′, Pmax, and PWD are 0.0267, 0.0174, 0.0011, and 0.0163, respectively.
Cited by 1 articles
-
Echocardiographic Evaluation of Right-sided Heart in Pediatric Patients with Adenotonsillar Hypertrophy
Sung Hye Kim
J Cardiovasc Imaging. 2018;26(4):214-216. doi: 10.4250/jcvi.2018.26.e30.
Reference
-
1. Duman D, Naiboglu B, Esen HS, Toros SZ, Demirtunc R. Impaired right ventricular function in adenotonsillar hypertrophy. Int J Cardiovasc Imaging. 2008; 24:261–267.
Article2. Attia G, Ahmad MA, Saleh AB, Elsharkawy A. Impact of obstructive sleep apnea on global myocardial performance in children assessed by tissue Doppler imaging. Pediatr Cardiol. 2010; 31:1025–1036.
Article3. Chan JY, Li AM, Au CT, et al. Cardiac remodelling and dysfunction in children with obstructive sleep apnoea: a community based study. Thorax. 2009; 64:233–239.
Article4. Kocabaş A, Salman N, Ekici F, Cetin I, Akcan FA. Evaluation of cardiac functions and atrial electromechanical delay in children with adenotonsillar hypertrophy. Pediatr Cardiol. 2014; 35:785–792.
Article5. Lee JH, Yoon JM, Lim JW, et al. Effect of adenotonsillar hypertrophy on right ventricle function in children. Korean J Pediatr. 2014; 57:484–488.
Article6. Luijnenburg SE, Peters RE, van der Geest RJ, et al. Abnormal right atrial and right ventricular diastolic function relate to impaired clinical condition in patients operated for tetralogy of Fallot. Int J Cardiol. 2013; 167:833–839.
Article7. Moceri P, Dimopoulos K, Liodakis E, et al. Echocardiographic predictors of outcome in eisenmenger syndrome. Circulation. 2012; 126:1461–1468.
Article8. Pirat B, Khoury DS, Hartley CJ, et al. A novel feature-tracking echocardiographic method for the quantitation of regional myocardial function: validation in an animal model of ischemia-reperfusion. J Am Coll Cardiol. 2008; 51:651–659.9. Gaisl T, Wons AM, Rossi V, et al. Simulated obstructive sleep apnea increases P-wave duration and P-wave dispersion. PLoS One. 2016; 11:e0152994.
Article10. Brodsky L, Moore L, Stanievich JF. A comparison of tonsillar size and oropharyngeal dimensions in children with obstructive adenotonsillar hypertrophy. Int J Pediatr Otorhinolaryngol. 1987; 13:149–156.
Article11. Lee CH, Kim YJ, Lee SB, Yoo CK, Kim HM. Psychological screening for the children with habitual snoring. Int J Pediatr Otorhinolaryngol. 2014; 78:2145–2150.
Article12. Fujioka M, Young LW, Girdany BR. Radiographic evaluation of adenoidal size in children: adenoidal-nasopharyngeal ratio. AJR Am J Roentgenol. 1979; 133:401–404.
Article13. Elwany S. The adenoidal-nasopharyngeal ratio (AN ratio). Its validity in selecting children for adenoidectomy. J Laryngol Otol. 1987; 101:569–573.14. Chervin RD, Hedger K, Dillon JE, Pituch KJ. Pediatric sleep questionnaire (PSQ): validity and reliability of scales for sleep-disordered breathing, snoring, sleepiness, and behavioral problems. Sleep Med. 2000; 1:21–32.
Article15. Redline S, Amin R, Beebe D, et al. The Childhood Adenotonsillectomy Trial (CHAT): rationale, design, and challenges of a randomized controlled trial evaluating a standard surgical procedure in a pediatric population. Sleep. 2011; 34:1509–1517.
Article16. Lopez L, Colan SD, Frommelt PC, et al. Recommendations for quantification methods during the performance of a pediatric echocardiogram: a report from the Pediatric Measurements Writing Group of the American Society of Echocardiography Pediatric and Congenital Heart Disease Council. J Am Soc Echocardiogr. 2010; 23:465–495. quiz 576-7.
Article17. Levy PT, Patel MD, Groh G, et al. Pulmonary artery acceleration time provides a reliable estimate of invasive pulmonary hemodynamics in children. J Am Soc Echocardiogr. 2016; 29:1056–1065.
Article18. Hou J, Yu HK, Wong SJ, Cheung YF. Atrial mechanics after surgical repair of tetralogy of Fallot. Echocardiography. 2015; 32:126–134.
Article19. Kang SJ, Kwon YW, Hwang SJ, Kim HJ, Jin BK, Yon DK. Clinical utility of left atrial strain in children in the acute phase of Kawasaki disease. J Am Soc Echocardiogr. 2018; 31:323–332.
Article20. Can I, Aytemir K, Demir AU, et al. P-wave duration and dispersion in patients with obstructive sleep apnea. Int J Cardiol. 2009; 133:e85–9.
Article21. Cagirci G, Cay S, Gulsoy KG, et al. Tissue Doppler atrial conduction times and electrocardiogram interlead P-wave durations with varying severity of obstructive sleep apnea. J Electrocardiol. 2011; 44:478–482.
Article22. Magnani JW, Williamson MA, Ellinor PT, Monahan KM, Benjamin EJ. P wave indices: current status and future directions in epidemiology, clinical, and research applications. Circ Arrhythm Electrophysiol. 2009; 2:72–79.23. Kutty S, Padiyath A, Li L, et al. Functional maturation of left and right atrial systolic and diastolic performance in infants, children, and adolescents. J Am Soc Echocardiogr. 2013; 26:398–409.e2.
Article24. Blume GG, Mcleod CJ, Barnes ME, et al. Left atrial function: physiology, assessment, and clinical implications. Eur J Echocardiogr. 2011; 12:421–430.
Article25. Padeletti M, Cameli M, Lisi M, et al. Right atrial speckle tracking analysis as a novel noninvasive method for pulmonary hemodynamics assessment in patients with chronic systolic heart failure. Echocardiography. 2011; 28:658–664.
Article26. Barbier P, Solomon SB, Schiller NB, Glantz SA. Left atrial relaxation and left ventricular systolic function determine left atrial reservoir function. Circulation. 1999; 100:427–436.
Article27. Okumura K, Slorach C, Mroczek D, et al. Right ventricular diastolic performance in children with pulmonary arterial hypertension associated with congenital heart disease: correlation of echocardiographic parameters with invasive reference standards by high-fidelity micromanometer catheter. Circ Cardiovasc Imaging. 2014; 7:491–501.28. Sanner BM, Konermann M, Sturm A, Müller HJ, Zidek W. Right ventricular dysfunction in patients with obstructive sleep apnoea syndrome. Eur Respir J. 1997; 10:2079–2083.
Article29. Shivalkar B, Van de Heyning C, Kerremans M, et al. Obstructive sleep apnea syndrome: more insights on structural and functional cardiac alterations, and the effects of treatment with continuous positive airway pressure. J Am Coll Cardiol. 2006; 47:1433–1439.30. Ostman-Smith I. Cardiac sympathetic nerves as the final common pathway in the induction of adaptive cardiac hypertrophy. Clin Sci (Lond). 1981; 61:265–272.31. Anversa P, Ricci R, Olivetti G. Quantitative structural analysis of the myocardium during physiologic growth and induced cardiac hypertrophy: a review. J Am Coll Cardiol. 1986; 7:1140–1149.
Article32. Gami AS, Hodge DO, Herges RM, et al. Obstructive sleep apnea, obesity, and the risk of incident atrial fibrillation. J Am Coll Cardiol. 2007; 49:565–571.
Article33. Sade LE, Gulmez O, Eroglu S, Sezgin A, Muderrisoglu H. Noninvasive estimation of right ventricular filling pressure by ratio of early tricuspid inflow to annular diastolic velocity in patients with and without recent cardiac surgery. J Am Soc Echocardiogr. 2007; 20:982–988.34. D'hooge J, Heimdal A, Jamal F, et al. Regional strain and strain rate measurements by cardiac ultrasound: principles, implementation and limitations. Eur J Echocardiogr. 2000; 1:154–170.35. Nageh MF, Kopelen HA, Zoghbi WA, Quiñones MA, Nagueh SF. Estimation of mean right atrial pressure using tissue Doppler imaging. Am J Cardiol. 1999; 84:1448–1451. A8
Article36. Mitchell RB. Adenotonsillectomy for obstructive sleep apnea in children: outcome evaluated by pre- and postoperative polysomnography. Laryngoscope. 2007; 117:1844–1854.
Article37. Marcus CL, Brooks LJ, Draper KA, et al. Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics. 2012; 130:576–584.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Weight Change in Young Children after Adenotonsillectomy
- The Effects of Adenotonsillectomy on Weight Change in Young Children
- Electrocardiographic Findings in School Children
- Impact of Adenotonsillar Hypertrophy on Child Personality and Behavior
- Effect of adenotonsillar hypertrophy on snoring in children
