Dimensional changes in reconstructed nipples: autologous versus prosthetic breast reconstruction
- Affiliations
-
- 1Department of Plastic & Reconstructive Surgery, Institute for Human Tissue Restoration, Yonsei University College of Medicine, Seoul, Korea. xyphoss@yuhs.ac
- KMID: 2429748
- DOI: http://doi.org/10.4174/astr.2019.96.1.8
Abstract
- PURPOSE
The creation of the nipple-areola complex is the final stage in breast reconstruction and highly affects patient satisfaction. The neo-nipple is well known to shrink over time, particularly in the nipple projection. Currently, no reconstruction technique is clearly superior in terms of nipple size maintenance. We evaluated nipple size changes among several methods of breast mound reconstruction.
METHODS
Seventy-eight patients received nipple-areola complex reconstruction secondarily after breast reconstruction. C-V flap nipple reconstructions were performed using a free transverse rectus abdominis myocutaneous (TRAM) flap in 25 cases (TRAM group), a latissimus dorsi (LD) myocutaneous flap in 27 cases (LD group), and an implant in 26 cases (implant group). The circumference and projection of the neo-nipple were measured using a flexible ruler, immediately after reconstruction and average 10 months after surgery.
RESULTS
The overall circumference and projection at the final measurement were 91.43% ± 7.11% and 62.16% ± 21.55%, respectively, of immediate postoperative values. The change in circumference did not significantly differ among the 3 groups. In contrast, the change in projection was significantly worse in implant group compared to that in TRAM and LD groups. In addition, among the patients in implant group, greater inflation was significantly associated with greater decrease in the nipple projection.
CONCLUSION
Breast mound reconstruction with autologous musculocutaneous flap techniques achieves better long-term maintenance of the neo-nipple projection compared to that achieved with expanded tissue and implantation. Considering the prospective loss of long-term nipple dimension, the preoperative design should be oversized in accordance with its origin in mound reconstruction.
MeSH Terms
Figure
-
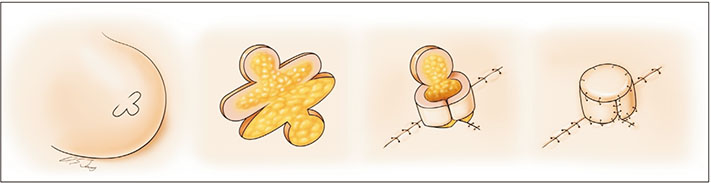
Fig. 1 Nipple reconstruction using a modified C-V flap technique. One C flap and 2 rounded V-flaps were elevated from the reconstructed breast mound while preserving dermis and fat tissue. After thinning of subcutaneous fat tissue, bilateral wings of the rounded V-flap were sutured with nylon. The C-flap and V-flap donor sites were closed primarily.

Fig. 2 Comparison of the change in nipple circumference and projection among various reconstruction methods. Nipples from autologous tissue showed more stability than nipples from expanded tissue. *P < 0.05.
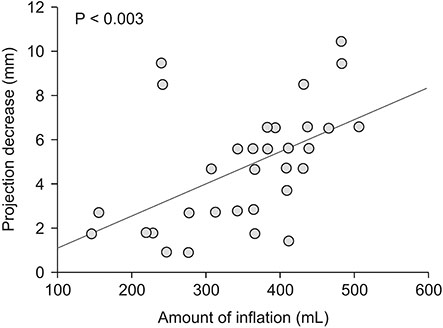
Fig. 3 Pearson correlations and scatterplot depicting the relationship between expansion and nipple projection changes among the patients in implant group. In group C, as the amount of postoperative expansion increases, the rate of projection decrease is greater (P < 0.003).
Reference
-
1. Chang JM, Kosiorek HE, Dueck AC, Casey WJ, Rebecca AM, Mahabir R, et al. Trends in mastectomy and reconstruction for breast cancer; a twelve year experience from a tertiary care center. Am J Surg. 2016; 212:1201–1210.
Article2. Mota BS, Riera R, Ricci MD, Barrett J, de Castria TB, Atallah ÁN, et al. Nipple- and areola-sparing mastectomy for the treatment of breast cancer. Cochrane Database Syst Rev. 2016; 11:CD008932.
Article3. Wellisch DK, Schain WS, Noone RB, Little JW 3rd. The psychological contribution of nipple addition in breast reconstruction. Plast Reconstr Surg. 1987; 80:699–704.
Article4. Shestak KC, Gabriel A, Landecker A, Peters S, Shestak A, Kim J. Assessment of long-term nipple projection: a comparison of three techniques. Plast Reconstr Surg. 2002; 110:780–786.
Article5. Few JW, Marcus JR, Casas LA, Aitken ME, Redding J. Long-term predictable nipple projection following reconstruction. Plast Reconstr Surg. 1999; 104:1321–1324.6. Kroll SS, Reece GP, Miller MJ, Evans GR, Robb GL, Baldwin BJ, et al. Comparison of nipple projection with the modified double-opposing tab and star flaps. Plast Reconstr Surg. 1997; 99:1602–1605.
Article7. Banducci DR, Le TK, Hughes KC. Long-term follow-up of a modified Anton-Hartrampf nipple reconstruction. Ann Plast Surg. 1999; 43:467–469.
Article8. Yun IS, Lew DH, Tark KC. Nipple Reconstruction with Modified C-V Flap: C-U Flap. J Korean Soc Aesthetic Plast Surg. 2008; 14:75–78.9. Kroll SS, Hamilton S. Nipple reconstruction with the double-opposing-tab flap. Plast Reconstr Surg. 1989; 84:520–525.
Article10. Losken A, Mackay GJ, Bostwick J 3rd. Nipple reconstruction using the C-V flap technique: a long-term evaluation. Plast Reconstr Surg. 2001; 108:361–369.
Article11. El-Ali K, Dalal M, Kat CC. Modified C-V flap for nipple reconstruction: our results in 50 patients. J Plast Reconstr Aesthet Surg. 2009; 62:991–996.
Article12. Mori H, Hata Y. Modified C-V flap in nipple reconstruction. J Plast Reconstr Aesthet Surg. 2008; 61:1109–1110.
Article13. Eo S, Kim SS, Da Lio AL. Nipple reconstruction with C-V flap using dermofat graft. Ann Plast Surg. 2007; 58:137–140.
Article14. Zhong T, Antony A, Cordeiro P. Surgical outcomes and nipple projection using the modified skate f lap for nipple-areolar reconstruction in a series of 422 implant reconstructions. Ann Plast Surg. 2009; 62:591–595.15. Eskenazi L. A one-stage nipple reconstruction with the “modified star” flap and immediate tattoo: a review of 100 cases. Plast Reconstr Surg. 1993; 92:671–680.16. Little JW 3rd. Nipple-areola reconstruction. Clin Plast Surg. 1984; 11:351–364.
Article17. Heitland A, Markowicz M, Koellensperger E, Allen R, Pallua N. Long-term nipple shrinkage following augmentation by an autologous rib cartilage transplant in free DIEP-flaps. J Plast Reconstr Aesthet Surg. 2006; 59:1063–1067.
Article18. Brent B, Bostwick J. Nipple-areola reconstruction with auricular tissues. Plast Reconstr Surg. 1977; 60:353–361.
Article19. Tanabe HY, Tai Y, Kiyokawa K, Yamauchi T. Nipple-areola reconstruction with a dermal-fat flap and rolled auricular cartilage. Plast Reconstr Surg. 1997; 100:431–438.
Article20. Guerra AB, Khoobehi K, Metzinger SE, Allen RJ. New technique for nipple areola reconstruction: arrow flap and rib cartilage graft for long-lasting nipple projection. Ann Plast Surg. 2003; 50:31–37.
Article21. Yanaga H. Nipple-areola reconstruction with a dermal-fat flap: technical improvement from rolled auricular cartilage to artificial bone. Plast Reconstr Surg. 2003; 112:1863–1869.22. Nahabedian MY. Secondary nipple reconstruction using local flaps and AlloDerm. Plast Reconstr Surg. 2005; 115:2056–2061.
Article23. Garramone CE, Lam B. Use of AlloDerm in primary nipple reconstruction to improve long-term nipple projection. Plast Reconstr Surg. 2007; 119:1663–1668.
Article24. Bernard RW, Beran SJ. Autologous fat graft in nipple reconstruction. Plast Reconstr Surg. 2003; 112:964–968.
Article25. Matturri L, Azzolini A, Riberti C, Lavezzi AM, Cavalca D, Vercesi F, et al. Long-term histopathologic evaluation of human expanded skin. Plast Reconstr Surg. 1992; 90:636–642.
Article26. Lee Y, Hwang K. Skin thickness of Korean adults. Surg Radiol Anat. 2002; 24:183–189.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Nipple Reconstruction using the C-V Flap Technique after Breast Reconstruction with the Only Breast Expander
- Plastic Surgery of the Breast
- Recent Knowledge of Breast Reconstruction
- Occurrence of contralateral breast cancer in a BRCA-positive breast cancer patient who underwent free TRAM flap reconstruction: a case report
- Immediate Nipple Reconstruction in Breast Reconstruction with TRAM Free Flap
